
Two days ago, the Gates Medical Research Institute and the Serum Institute of India announced an agreement to manufacture the M72/AS01E tuberculosis vaccine candidate, and Serum Institute committed to invest more than $100 million of its own resources in manufacturing readiness and capacity. Read as a headline, this is a clean story: the world's biggest vaccine maker by volume is finally backing a serious successor to the oldest vaccine still in routine use.
It is worth slowing down on both halves of that sentence. Today marks 105 years to the day since BCG was first given to a human being, on 18 July 1921, and BCG remains the only tuberculosis vaccine currently licensed and approved by the World Health Organization. And the trial that produced the evidence behind the vaccine Serum Institute has just agreed to manufacture never enrolled a single patient in India. Its Phase 3 study enrolled 20,000 participants across 54 sites in South Africa, Kenya, Malawi, Zambia and Indonesia, reaching full enrollment in April 2025 after starting in March 2024. That list of five countries does not include the one country carrying the largest share of the disease the vaccine is meant to fight.
A quarter of the world's cases, none of the trial's sites
India accounted for 25 percent of the world's incident tuberculosis cases in 2024, the largest national share on Earth and more than double Indonesia's, the next-largest at 10 percent.
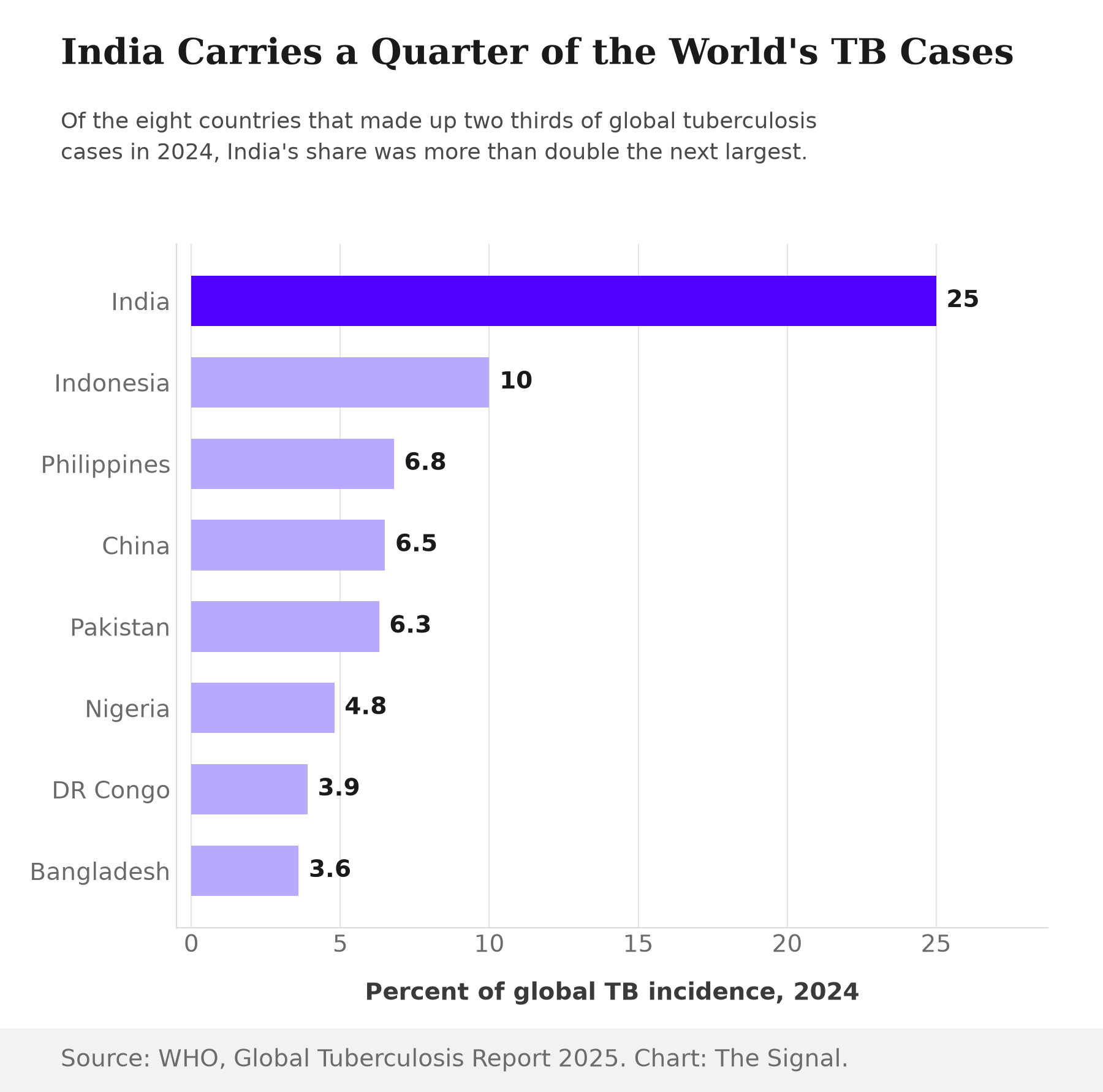
That is not a rounding gap: India's 25 percent alone outweighs Indonesia, the Philippines and China's shares combined (10 plus 6.8 plus 6.5, or 23.3 percent). And that trial enrolled its 20,000 participants in South Africa, Kenya, Malawi, Zambia and Indonesia, a list with no Indian site on it. Trial-site selection is a scientific and regulatory decision, not a popularity contest, and there are real reasons a sponsor might choose Sub-Saharan Africa and Indonesia over India for a Phase 3 tuberculosis study. But the plain fact stands: the evidence base for the vaccine Serum Institute will build was generated entirely outside the country the deal is anchored to.
One vaccine, 105 years old
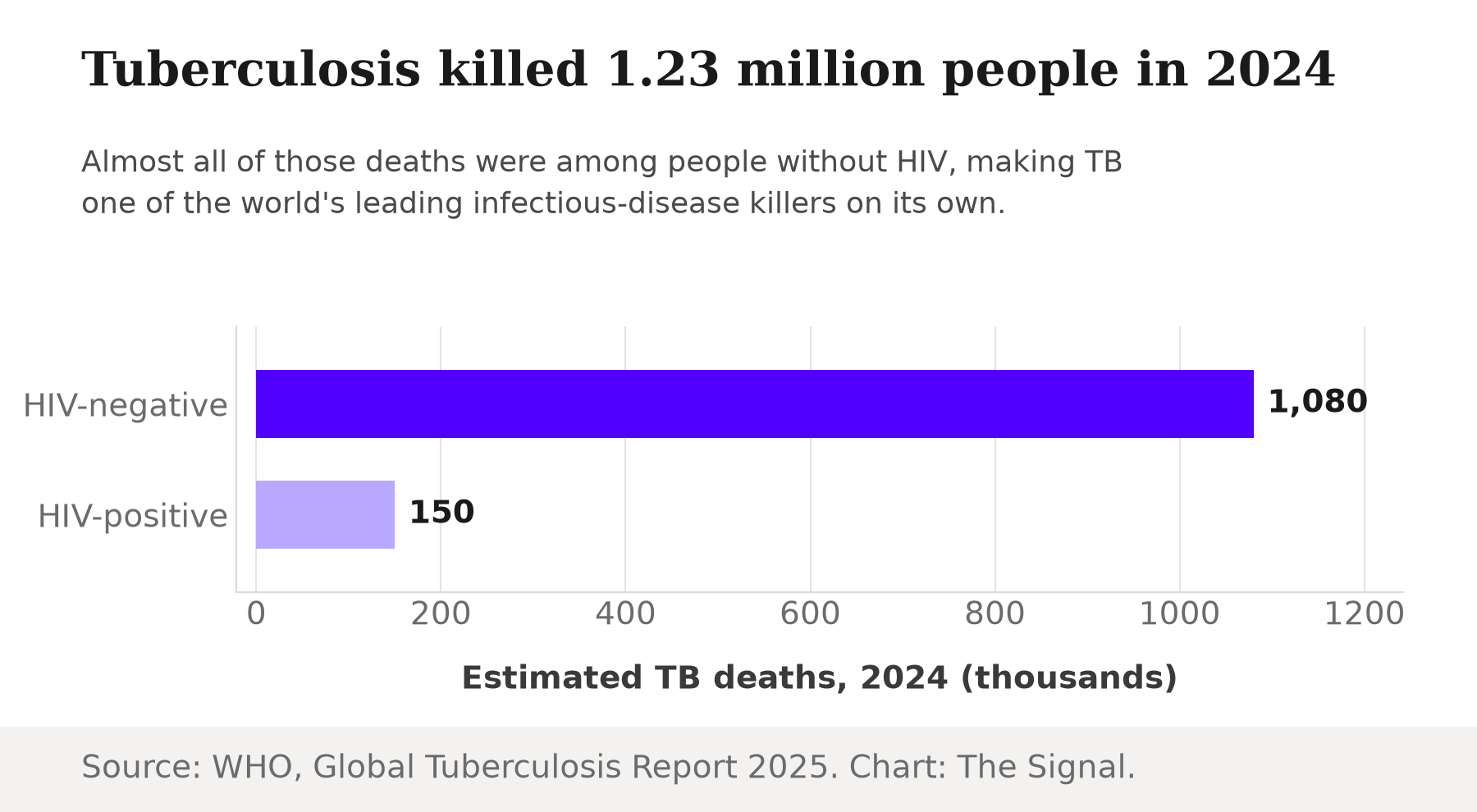
The reason a new vaccine matters is that the incumbent is not just old, it is essentially alone. Tuberculosis killed an estimated 1.23 million people worldwide in 2024, split between 1.08 million deaths among people without HIV and roughly 150,000 among people with HIV, and BCG has had no licensed peer since 1921.
A disease killing more than a million people a year, with one vaccine over a century old and imperfect against adult pulmonary disease, is exactly the kind of gap a company with Serum Institute's scale exists to close. Serum Institute sells more than 1.5 billion vaccine doses a year and holds a 28 percent share of all vaccine doses sold globally. That capacity has existed for years. What changed this month was not Serum Institute's ability to build the vaccine. It was who was paying to get it ready.
The capital came after Gates's, not before it
Serum Institute's more-than-$100-million manufacturing commitment sits inside an agreement structured and funded by the Gates Medical Research Institute, the Gates Foundation's nonprofit clinical-research arm. Gates MRI sponsored the Phase 3 trial, ran it in five countries that were not India, and its agreement, not Serum Institute's own initiative, put a manufacturing timeline on the calendar this week.
That is a revealing order of operations. Serum Institute, selling more than 1.5 billion doses a year, did not need anyone's permission to invest in tuberculosis manufacturing capacity for a country carrying a quarter of the global caseload. It moved once a foreign philanthropic nonprofit had already run the trial and structured the manufacturing deal. Manufacturing readiness is real and valuable. It is also the easier half of the problem, and it is the half that arrived last.
What a working vaccine is actually worth
54.0 percent is a real number, not statistical noise. In the Phase 2b trial of 3,575 randomized adults, M72/AS01E showed 54.0 percent efficacy against active pulmonary TB after a mean follow-up of 2.3 years, the result that justified running the larger Phase 3 study at all. WHO modelling finds that a vaccine effective just 50 percent of the time, below the 54.0 percent already shown, could avert up to 76 million TB cases, 8.5 million deaths and $42 billion in household costs over 25 years if approved and scaled rapidly.
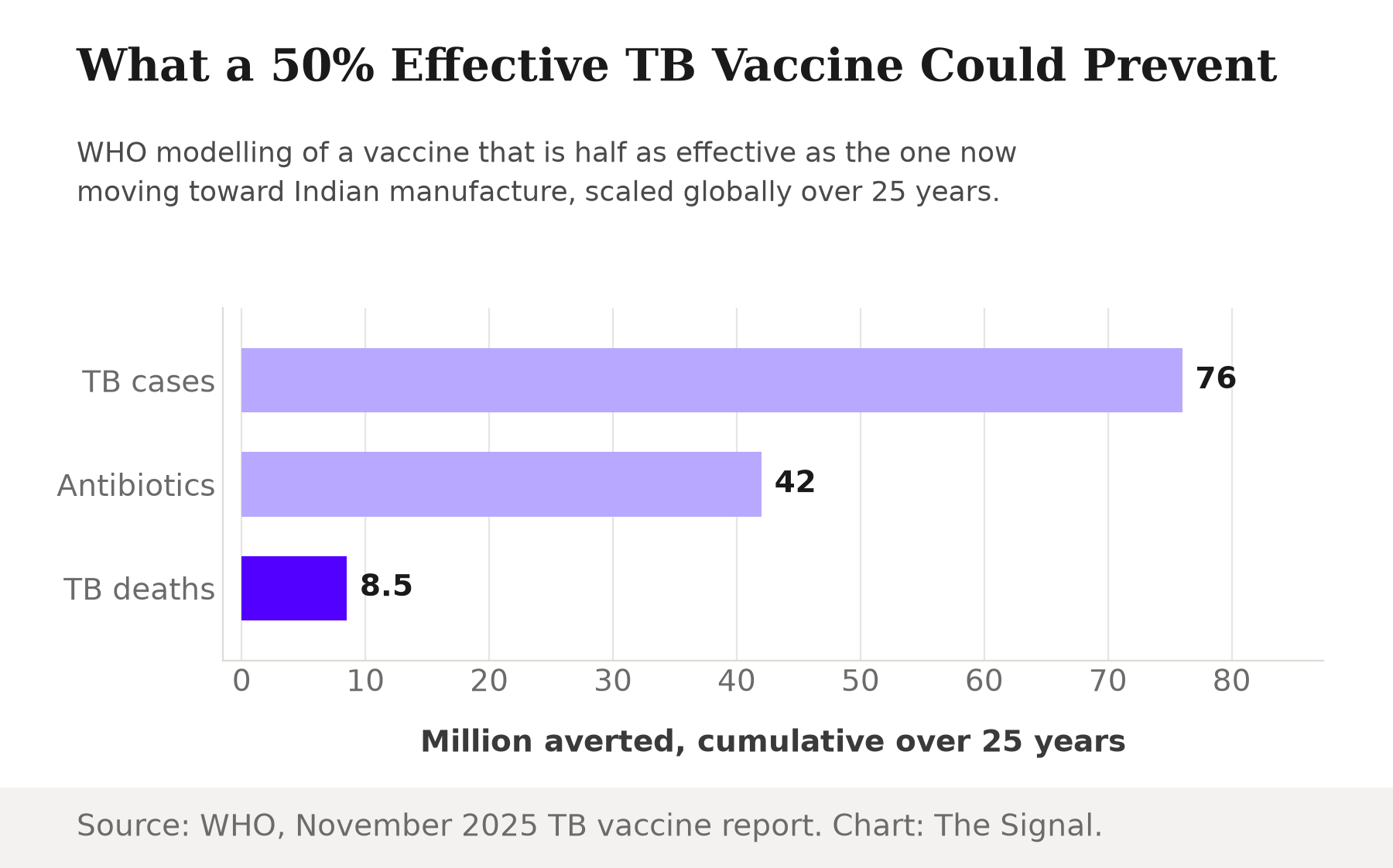
Those figures are global, not India-specific, because that is what WHO modelled. But a country supplying a quarter of the world's cases captures a large, undefined share of whichever slice of that 76 million and 8.5 million actually materializes, which is the entire reason a vaccine manufactured in India, tested for evidence generated abroad, still matters enormously to India.
The honest objection
The strongest case against reading anything into the trial's geography is that Phase 3 tuberculosis trials chase infrastructure and speed, not headlines. A trial can reach a statistically meaningful result faster where HIV-TB coinfection is common enough to concentrate cases in a smaller population, and a single-regulator market like Indonesia can move faster than India's more complex multi-agency approval process. On this reading, Serum Institute is not late to caring about tuberculosis. India's own National Tuberculosis Elimination Programme set a target of ending TB by 2025, five years ahead of the global 2030 deadline, pursued through expanded testing and treatment rather than a new vaccine, so a manufacturing deal signed after the trial data existed is simply how vaccine adoption normally works everywhere.
That case is real, and trial-site logistics are not evidence of neglect. But it does not explain the second half of the pattern: Serum Institute's own capital commitment only arrived once someone else had de-risked the science. A domestic manufacturer with 1.5 billion doses of annual capacity did not need to wait for outside money to start planning for a disease that kills more people in its home market than almost anywhere else. It waited anyway. And India's 2025 elimination target, cited as the domestic alternative to a vaccine push, is itself now a year and a half in the past: India's own count shows TB incidence falling 21 percent since 2015, from 237 to 187 cases per lakh population, roughly double the pace of the global decline but nowhere near the elimination the deadline implied, with no vaccine yet in Indian arms.
The Signal
This deal is genuinely good news: a vaccine candidate already shown to be 54.0 percent efficacious is finally moving toward manufacture at the scale a disease this size demands. But the sequence that produced it says something sharper than the announcement does. The country with the largest share of the world's tuberculosis contributed no trial sites and, until this week, no capital of its own to the vaccine now bound for its factories. Watch what happens after the Phase 3 results read out. Serum Institute's doses reaching India on terms India helped set would make this week's deal the start of India steering its own tuberculosis response. If India's role stays limited to manufacturing what a foreign nonprofit already proved, the country that carries the disease will still not be the country that decides how it gets fought.
Reporting basis: TB incidence and mortality figures for 2024 are from the WHO's Global Tuberculosis Report 2025. BCG's status as the sole licensed vaccine and its 1921 origin come from a peer-reviewed review in Vaccines. The Gates MRI-Serum Institute manufacturing agreement and the Phase 3 trial's enrollment, sites and dates are per Gates Medical Research Institute's own announcement, the trial's sponsor. Serum Institute's investment commitment is as reported by ThePrint. The Phase 2b efficacy result is from the trial's original report in the New England Journal of Medicine. The vaccine-impact modelling is from WHO's November 2025 report on equitable access to TB vaccines. Serum Institute's production scale and market share are from a peer-reviewed article in the Journal of Commercial Biotechnology. India's National Tuberculosis Elimination Programme target is from a Press Information Bureau release, and India's actual incidence and mortality decline since 2015 is from a separate Press Information Bureau release citing the WHO's Global Tuberculosis Report 2025. The 105-year gap since BCG's first human dose and the comparison of India's TB share against the next three largest countries combined are The Signal's calculations from those figures.


