
Two countermeasures against the same outbreak went into use within a day of each other this month. On July 14, 2026, the WHO-backed EBO-PEP trial began testing Gilead's antiviral obeldesivir as post-exposure prophylaxis in Ituri province, Democratic Republic of Congo, aiming to enroll nearly 1,000 participants aged 12 and over who had high-risk contact with a confirmed case in the preceding five days, per Africa CDC. A day earlier, the Serum Institute of India had already manufactured and stockpiled roughly 620,000 doses of an experimental Ebola vaccine in two weeks, supplying 4,000 of them to the vaccine's first human trial, CEPI reported. Read together, this looks like the global health system doing exactly what it exists to do: mobilizing fast against a lethal outbreak.
It is worth slowing down on what each effort is actually protecting against. The antiviral trial is running where the outbreak is. The vaccine stockpile is being built by a company on a different continent, for a country that does not need it. India has not reported a single case of Bundibugyo Ebola disease, the government said as it stepped up surveillance after the World Health Organization's emergency declaration. Not one, ever.
The stockpile dwarfs the trial that produced it, and nothing yet confirms the world will ever need it.
The shot nobody in India will get
The vaccine candidate is a joint effort: CEPI committed initial funding of up to US$8.6 million to the University of Oxford and the Serum Institute of India to fund preclinical testing and rapidly prepare a Phase 1 trial of a vaccine built on Oxford's ChAdOx1 platform, the same viral-vector platform that underpinned the Oxford/AstraZeneca Covid-19 vaccine. From that funding came a factory decision with an unusual shape: SII manufactured and stockpiled approximately 620,000 doses of the ChAdOx1 BDBV candidate in two weeks, and supplied only 4,000 investigational doses to the Phase 1 trial itself.
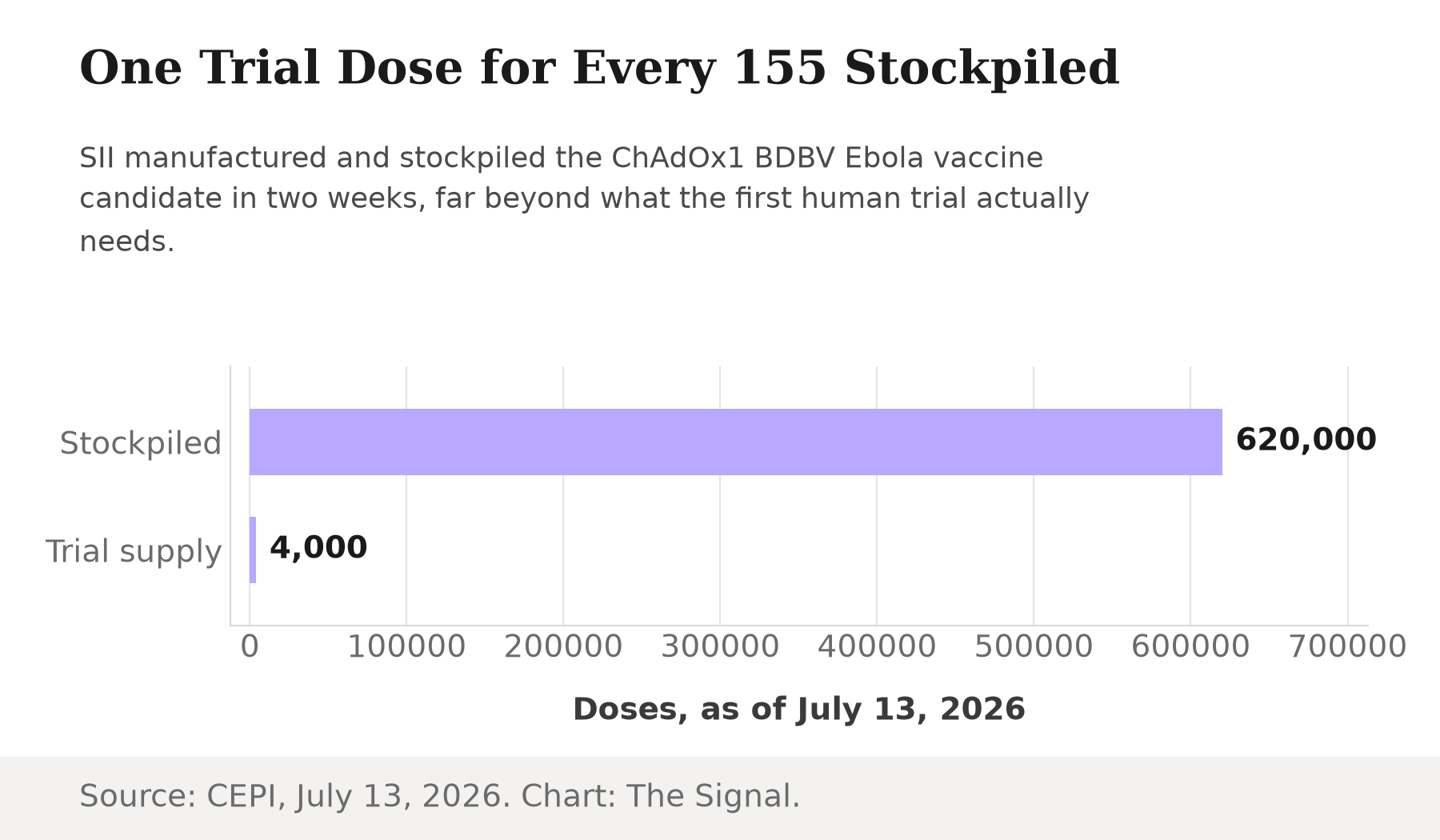
That is a stockpile built for a decision that has not yet been made. Phase 1 trials exist to answer whether a vaccine is safe and generates an immune response, not whether it works in the field. SII built out manufacturing capacity for an outbreak response before that question was answered, which is either remarkably fast preparedness or a company that has already decided it wants to be the name attached to the eventual answer.
An outbreak that keeps outrunning its own case count
The outbreak driving all of this began in Ituri province. DRC's Ministry of Public Health officially declared the country's 17th Ebola Disease outbreak on 15 May 2026, ten days after WHO was first alerted to a cluster of high-mortality illness there. Two days later, WHO's Director-General determined the Bundibugyo virus outbreak in DRC and Uganda a Public Health Emergency of International Concern, the WHO's highest alarm level.
The case count has not slowed since. As of July 2, 2026, WHO counted 1,460 confirmed cases and 452 deaths in DRC, a crude case fatality ratio of 30.9%, plus 20 confirmed cases and two deaths in Uganda and one confirmed case in France: 1,481 cases and 454 deaths across all three countries. Eleven days later, on July 13, 2026, the ECDC put the outbreak's running total at 2,011 confirmed cases and 754 deaths.
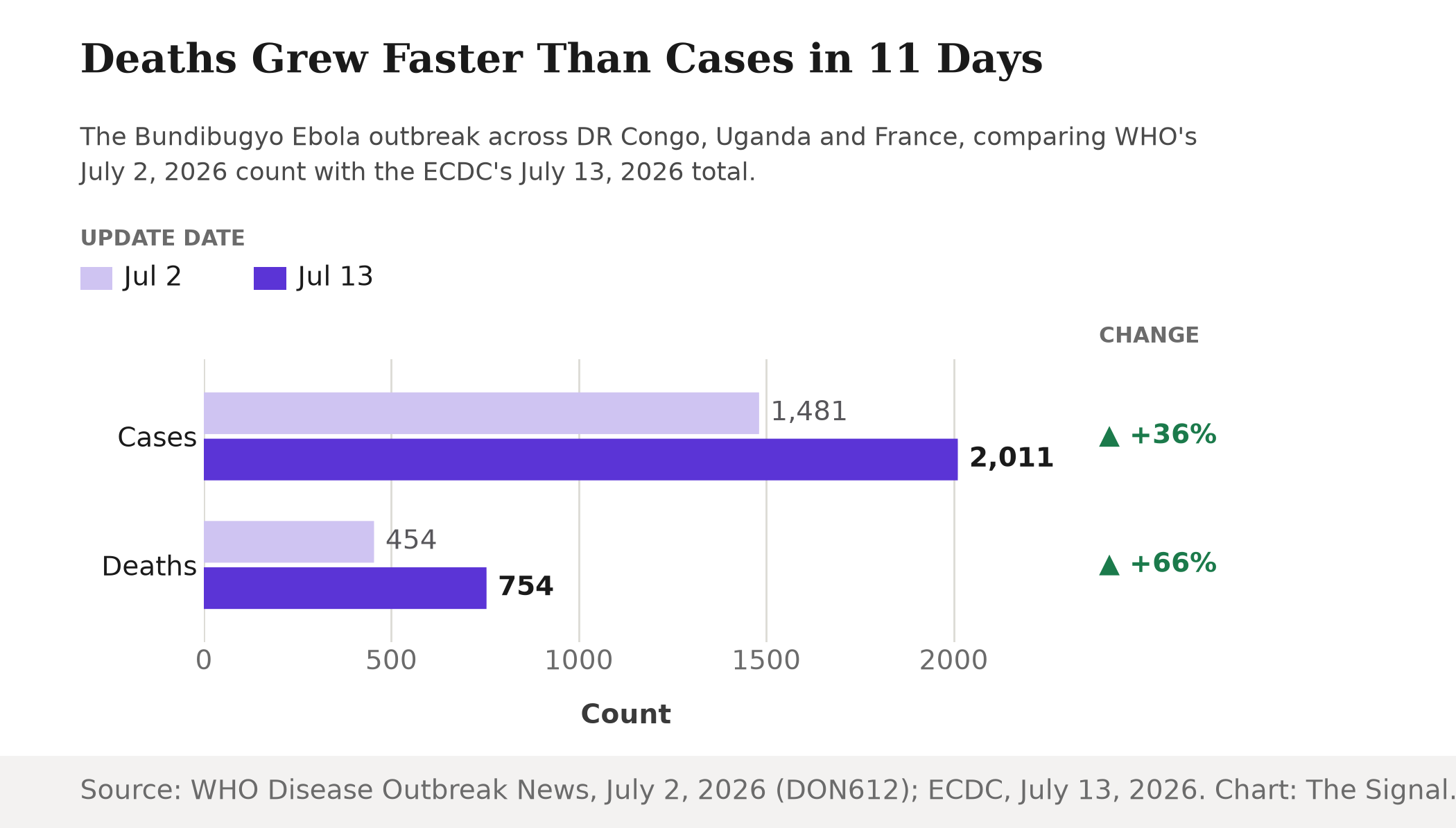
Deaths grew faster than cases in those eleven days, which is the kind of detail a stockpile decision has to be made against: nobody running a factory schedule gets to wait for a clean trend line. That is the case for urgency. It is not, on its own, the case for why the doses needed to be built in India specifically.
Zero cases, one manufacturer
Here is the gap the two efforts don't share. The antiviral trial serves the population living through the outbreak. The vaccine stockpile serves a company whose largest customer base has never seen the disease. SII sells more than 1.5 billion vaccine doses a year, and at least 65% of the world's children are immunized with at least one SII-made vaccine, according to a 2021 peer-reviewed profile in the Journal of Commercial Biotechnology, the most recent published estimate of that scale. Against that base, a 620,000-dose stockpile for one outbreak is a rounding error in production terms and a headline in reputational ones: expect that number to resurface in the next emergency, cited by whichever agency next decides who gets the contract to manufacture at speed.
| Metric | Figure | As of |
|---|---|---|
| Confirmed Ebola cases ever recorded in India | 0 | May 25, 2026 |
| Outbreak total, per ECDC | 2,011 confirmed cases, 754 deaths | July 13, 2026 |
| SII Ebola vaccine doses stockpiled | 620,000 | July 13, 2026 |
| SII's usual annual output, all vaccines | More than 1.5 billion doses | 2021 estimate |
Sources: PIB, ECDC, CEPI, Journal of Commercial Biotechnology. Compiled by The Signal.
This is the same playbook SII ran during Covid-19: use spare manufacturing capacity and an established Oxford partnership to become the supplier of choice for a shot the rest of the world needs urgently and India did not need at the same moment on the same terms. The company is not curing a disease at home. It is renewing a claim on being ready the next time a hemorrhagic fever crosses a border and a manufacturer is needed on short notice.
The honest objection
The strongest case against reading this as a diplomacy play is that this is exactly what a responsible vaccine manufacturer with SII's scale should be doing. CEPI's entire model exists to compress the years between an outbreak and a deployable vaccine into months, and that depends on a manufacturer willing to build stock ahead of a confirmed efficacy signal, before demand is proven, on the expectation that the emergency does not wait for paperwork. A company that already immunizes 65% of the world's children arguably carries a standing global-health obligation that has nothing to do with whether the disease has ever touched its home market.
That case is real, and it is why CEPI exists. But it does not explain the scale of the bet. A precautionary stockpile ahead of a safety readout is standard practice; 620,000 doses against a trial of 4,000, a ratio of 155 to 1, is a wager that this specific vaccine, from this specific manufacturer, becomes the one the world reaches for. There is a real-world base rate for how long that wager can take to pay off: WHO did not prequalify an Ebola vaccine for the first time until 12 November 2019, roughly three years after the 2014-2016 West Africa epidemic that drove its development had ended. A vaccine can outlast the outbreak it was built for by years before it becomes a licensed, purchasable product. If the outbreak is brought under control by the antiviral trial, by containment, or simply by burning through susceptible contacts before Phase 1 data even reads out, those doses have no other buyer: the disease they were built for has never existed anywhere they could otherwise be sold. As of 29 May 2026, Gavi had committed up to $50 million to the outbreak response and was still only exploring an advance purchase commitment for a Bundibugyo vaccine with CEPI, not finalizing one: the stockpile currently has funding interest behind it, not a signed order.
The Signal
Strip away the emergency framing and what is left is a manufacturing and reputation bet, not a public health response to a domestic threat. Africa CDC's antiviral trial and the emergency declaration that triggered it answer to the outbreak in front of them. Serum Institute's 620,000 doses answer to the outbreak after this one, and the one after that, wherever it lands. The number to watch is not the case count in DRC. It is whether Phase 1 immunogenicity data reads out, and whether any global buyer signs a purchase order, before this outbreak resolves on its own. A stockpile with no order behind it is not a safety net. It is inventory.
Reporting basis: the Africa CDC report is the origin for the EBO-PEP antiviral trial's launch and enrollment criteria. CEPI is the origin for its own funding commitment and for the Serum Institute of India's manufacturing and trial-supply figures, both drawn from CEPI's own announcements. The outbreak's declaration and Public Health Emergency of International Concern status are per the World Health Organization's Disease Outbreak News and its own PHEIC determination. The July 2, 2026 case and death counts are from the World Health Organization's Disease Outbreak News; the July 13, 2026 total is a separate, independent count from the European Centre for Disease Prevention and Control, not a recarry of the earlier figure. India's zero-case status is per a Press Information Bureau release citing the Union Ministry of Health and Family Welfare. The Serum Institute's annual manufacturing scale rests on a single 2021 peer-reviewed estimate in the Journal of Commercial Biotechnology; no newer figure was available. The rVSV-ZEBOV prequalification date is per WHO's own prequalification team. The status of any advance purchase commitment is per Gavi's own May 29, 2026 announcement of its funding commitment. The three-country outbreak totals for July 2, 2026, the three-year gap between that prequalification and the 2014-2016 outbreak that drove it, and the stockpile-to-trial ratio are all The Signal's calculations from those figures.


