
In June 2026, a Lancet series on chronic kidney disease put a number on a condition most people never think about until it fails. Chronic kidney disease affects an estimated 844 million adults worldwide, a University of Glasgow release on the research reports. Significant underdiagnosis of the disease, now the ninth leading cause of death globally, is set to matter more as it becomes the fifth leading cause by 2040, per a parallel release from the University of Liverpool. The reason so many cases go unmanaged is not a missing tool: a simple, affordable urine test can detect the disease, but it is not routinely used across healthcare settings, Kidney Research UK reports on the same series.
That crisis has a narrow, expensive tail. Globally, only about 4 million of the roughly 850 million people living with some stage of chronic kidney disease need kidney replacement therapy (dialysis or a transplant) for kidney failure, the underlying Lancet paper's abstract states. Most chronic kidney disease, caught in time, does not have to end there. The disease that reaches failure is disproportionately the disease nobody caught early enough to manage.
India's own numbers on that gap are sharper than the global ones. In the SEEK-India screening study, only 7.9 percent of the people found to have chronic kidney disease knew they had it, and only 5.9 percent of those with protein in their urine were aware of it. That is not a wave still forming. It is a country where, by the time the disease is diagnosed, the overwhelming majority of cases have already gone unnoticed.
It is worth slowing down on that framing. The series describes a coming wave of undiagnosed kidney disease as though the world has not already run this experiment. India has. In the Uddanam belt of Andhra Pradesh, a population has spent two decades inside exactly the crisis the series describes: kidney disease that goes uncaught until it is a medical emergency. Uddanam already lived through that future, and the record of it still stands.
What Uddanam Already Shows
A 2020 study under the SEEK-Andhra research programme put CKD prevalence in Uddanam at 32.2 percent, against a national pooled prevalence of 13.24 percent found across Indian community studies published between 2011 and 2023, nearly two and a half times higher.
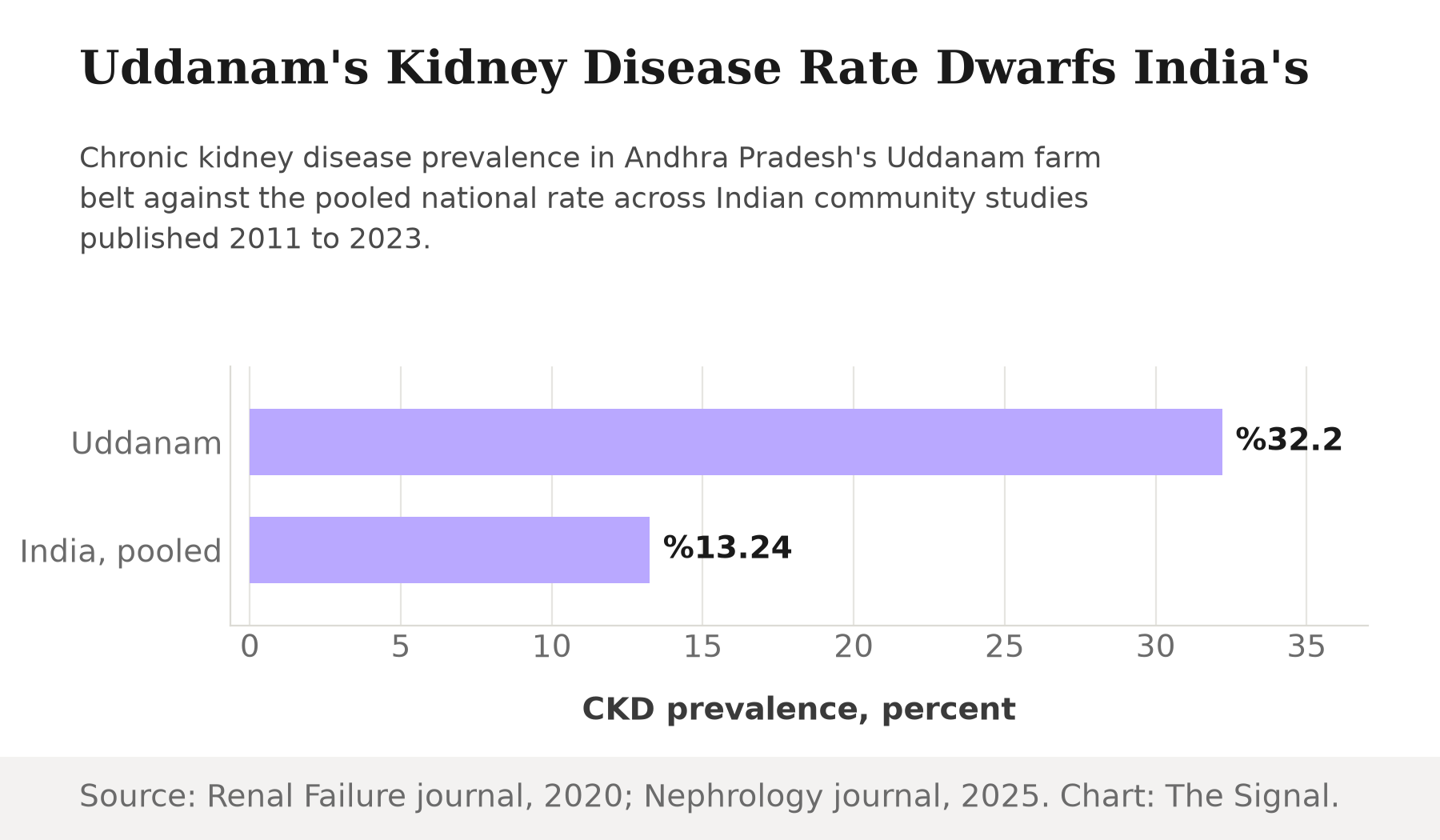
Source: Renal Failure journal, SEEK-Andhra study, 2020; Talukdar et al., Nephrology journal, 2025. Chart: The Signal.
The same SEEK-Andhra study found that working as a farmer carries a 20 percent higher CKD prevalence than non-farming occupations in the region. An earlier, starker estimate exists too. A 2017 epidemiological study put CKD of unknown etiology, CKDu, at 40 to 60 percent of Uddanam's population, nearly three times the national prevalence the study recorded at the time, with around 34,000 people affected and more than 4,500 deaths from the disease in the region in the decade to 2015.
Uddanam's kidney disease burden, by the numbers
| Measure | Figure | As of |
|---|---|---|
| CKD prevalence (SEEK-Andhra study) | 32.2% | 2020 study |
| CKD of unknown etiology (CKDu) | 40-60% of the population | 2015 |
| People affected by CKDu | About 34,000 | 2015 |
| Deaths attributed to CKD, decade to 2015 | More than 4,500 | 2015 |
Source: Renal Failure journal, SEEK-Andhra study, 2020; "Uddanam nephropathy in India: a challenge for epidemiologists", 2017.
Two different studies, three years apart, using different methods, arrive at the same conclusion from different angles: whatever the precise figure, Uddanam runs at multiples of India's own already-elevated national rate, and farming is the one occupational factor the data ties to more of it.
A System Built to Treat, Not Catch
India's national response to kidney failure is visible in a way its response to kidney disease itself is not. India adds about 2.2 lakh new end-stage renal disease patients every year, creating additional demand for 3.4 crore dialysis sessions annually, according to the Ministry of Health and Family Welfare. As of end-June 2026, the government's Pradhan Mantri National Dialysis Programme runs 1,856 centres with 13,535 hemodialysis machines across 751 districts in 36 states and union territories, and patients have availed 32.44 lakh dialysis services, with 432.29 lakh hemodialysis sessions held in total since the programme began.
Set those two figures side by side and the strain shows. The additional demand a single year of new patients creates, 3.4 crore dialysis sessions, is nearly as large as the 432.29 lakh sessions, about 4.32 crore, the entire national programme has delivered in total since it launched.
The buildout is still adding centres faster than it is closing the gap. As of 30 June 2025, a year before that dashboard snapshot, the programme had 1,704 dialysis centres functional across the same 751 districts, a Lok Sabha reply from the health ministry recorded. Centres grew by 152 in that single year, roughly 9 percent, while the number of districts covered did not move at all: geographic reach has plateaued, and the programme's growth is now in density, more machines per already-covered district, not in reaching new ground.
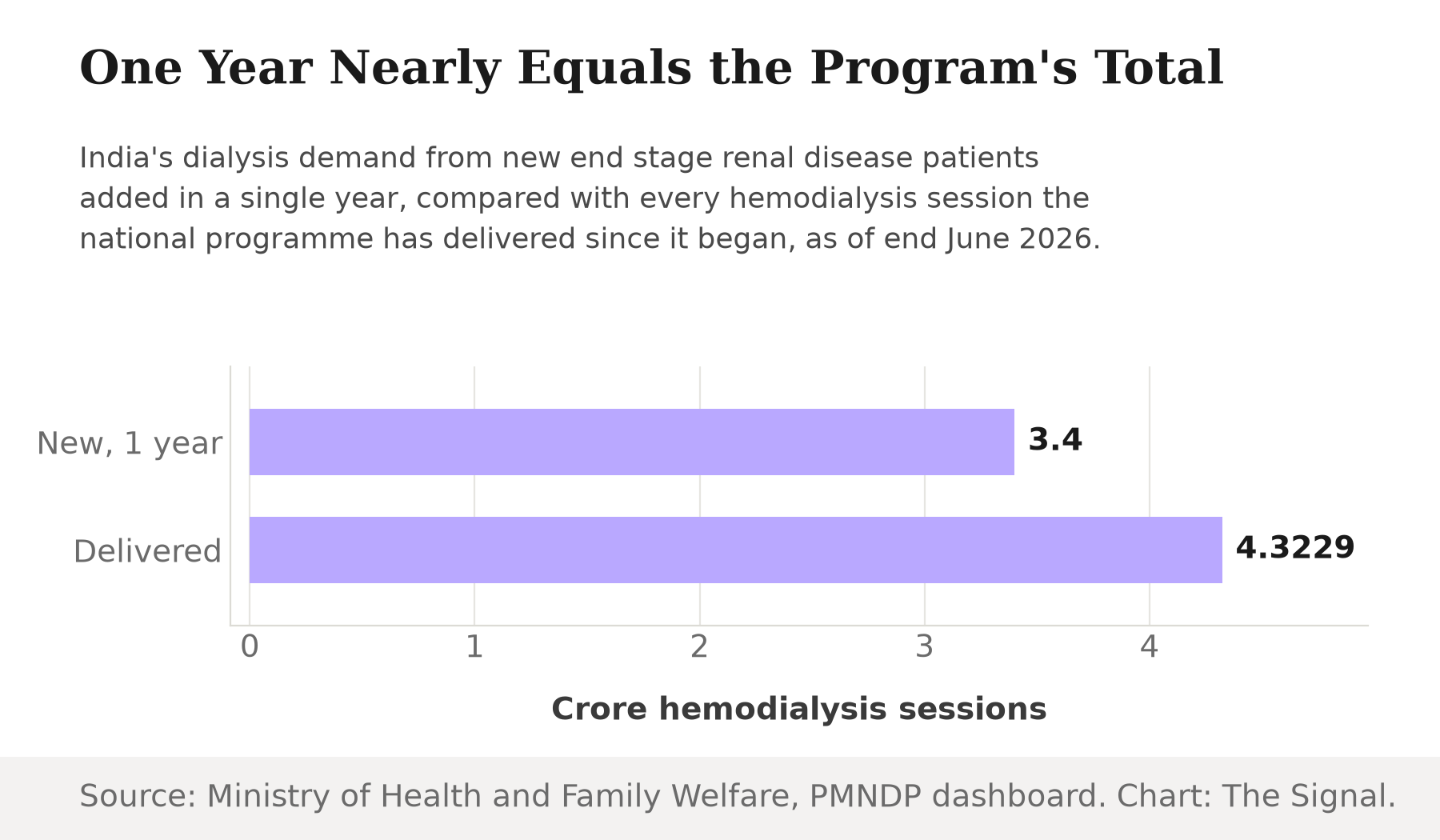
Source: Ministry of Health and Family Welfare, Pradhan Mantri National Dialysis Programme; PMNDP live dashboard. Chart: The Signal.
That reflects what a health system looks like when its main lever against kidney disease is treating failure rather than catching disease earlier, not a programme in crisis. The dashboard the ministry publishes counts centres, machines and sessions. It has no equivalent line for urine tests administered.
The bill for that choice falls on patients too. A 2018 costing study at a public-sector tertiary hospital found the average cost to the health system was about ₹4,148 per hemodialysis session, while patients paid a mean of ₹2,838 out of pocket for the same session.
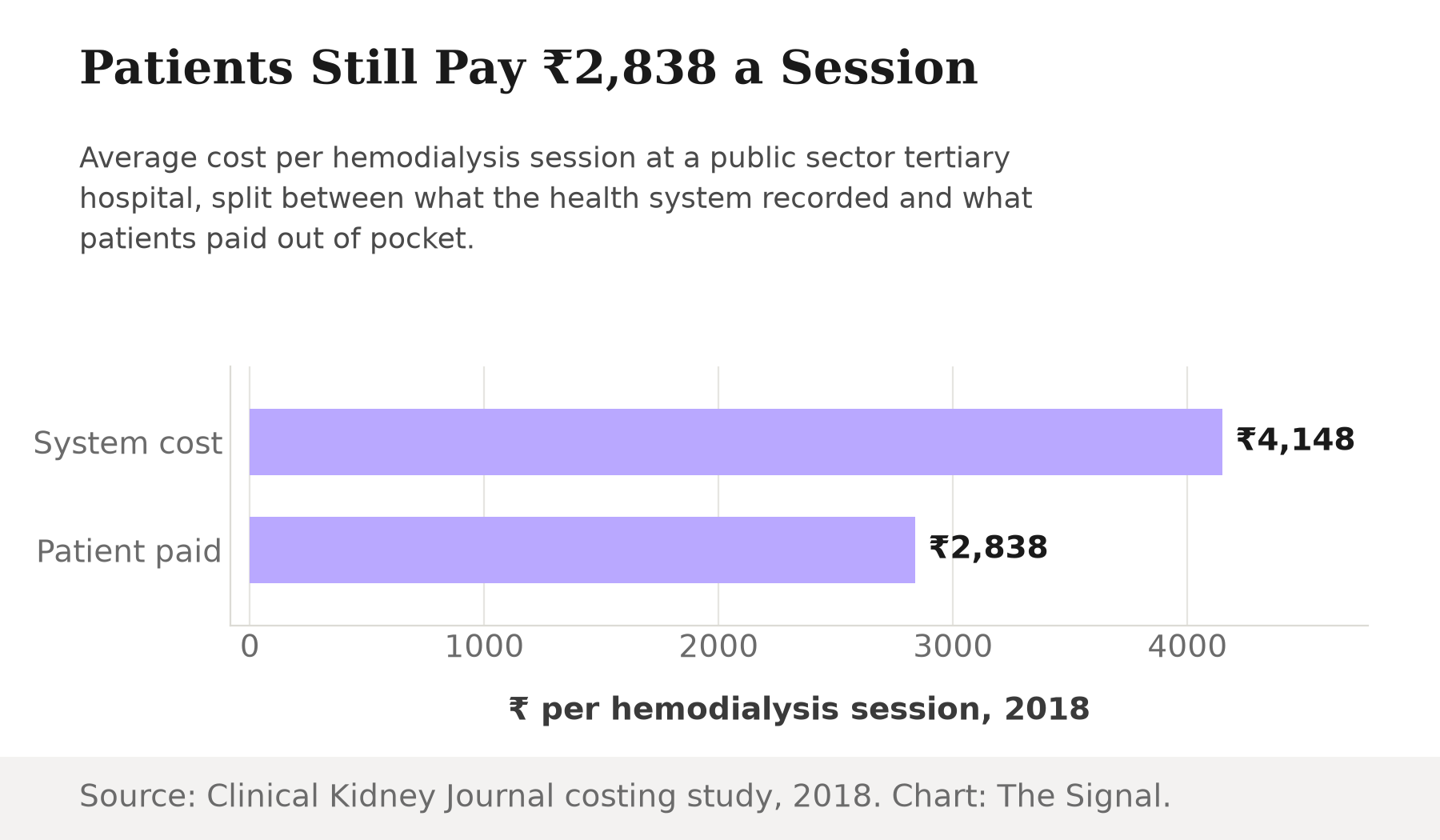
Source: Clinical Kidney Journal, costing study, 2018. Chart: The Signal.
Dialysis is typically needed multiple times a week, for as long as a patient stays on the programme, not once and done. A population caught only after its kidneys have already failed does not just cost more in aggregate. It hands each patient a recurring bill that early detection, using a test the Lancet series says is cheap and already exists, could have delayed or avoided.
The Honest Objection
The strongest case against blaming late diagnosis is that Uddanam's kidney disease may not be the kind a urine test alone fixes. Uddanam's disease is officially recorded as CKD of unknown etiology, and unknown etiology cuts both ways: if the trigger among Uddanam's farmers is environmental, in water quality, agrochemical exposure or repeated heat and dehydration, catching the disease earlier changes the treatment timeline but not necessarily the exposure that keeps producing new cases. There is at least a partial environmental lead: a 2020 groundwater study found lead levels above the safety limit in 55 percent of Uddanam villages sampled in the dry season, though even that finding, on its own, has not been established as the cluster's definitive cause. On this reading, the dialysis buildout is a rational response to a disease whose root cause research has not yet settled, not evidence of a system that skipped diagnosis.
That case has real force, but it does not extend to the national picture, only the regional one. Uddanam is an outlier even against India's own rising baseline, but the Lancet series' core claim is that underdiagnosis is a general property of kidney disease, not a feature specific to unexplained clusters like Uddanam's. A cheap, existing test would still catch the ordinary, well-understood cases, the hypertension-driven and diabetes-driven CKD that make up the bulk of India's growing pooled prevalence, whatever eventually explains Uddanam's harder-to-pin-down cluster.
The Signal
The world is being told to brace for a wave of undiagnosed kidney disease it has not yet fully counted. India does not need to brace. It has already spent a decade watching one farming belt run the entire arc: from undiagnosed disease, to a documented death toll, to a national programme built to dialyse the survivors. The lesson is not that Uddanam is exceptional. It is that a health system optimized to treat kidney failure, measured in centres, machines and sessions, will keep meeting patients exactly once, at the costliest, hardest-to-reverse point in the disease. The number worth watching next is not how many dialysis machines India adds, but whether a future dashboard update ever counts a urine test.
Reporting basis: the global prevalence and mortality-ranking figures are from a University of Glasgow release and a University of Liverpool release, both reporting on the same Lancet chronic kidney disease series published in June 2026, and the underused-urine-test point is per Kidney Research UK's release on that series. The figure for how many people need kidney replacement therapy is from the underlying Lancet paper's own abstract. The Uddanam prevalence figure and the farmer-occupation finding are from the peer-reviewed SEEK-Andhra paper published in Renal Failure in 2020; the CKDu prevalence range, the affected-population figure and the decade-to-2015 death toll are from a separate peer-reviewed epidemiological paper on Uddanam nephropathy published in 2017. India's pooled national CKD prevalence is from a 2025 systematic review and meta-analysis in the journal Nephrology. The CKD-awareness figures are from the peer-reviewed SEEK-India study published in BMC Nephrology in 2013. The dialysis demand and infrastructure figures are from the Ministry of Health and Family Welfare's Pradhan Mantri National Dialysis Programme page and live dashboard; the year-earlier centre count is from a Lok Sabha reply by the health ministry, reported by DD News. The Uddanam groundwater lead finding is from a 2020 study in the journal Groundwater for Sustainable Development, via TERI. The per-session cost figures are from a peer-reviewed 2018 costing analysis in the Clinical Kidney Journal. The comparison between one year's new dialysis demand and the programme's cumulative sessions delivered, and the year-over-year centre growth, are The Signal's calculations from those figures.


