
On July 13, 2026, Gujarat's health department, in a review chaired by health minister Praful Pansheriya, gave its latest count of the state's Chandipura virus outbreak. Of 27 suspected patients whose blood samples had been sent for testing, seven came back positive, twelve tested negative, and eight results were still awaited that evening. Three of the seven confirmed patients were already dead and four were under treatment, two each in Gandhinagar and Vadnagar in Mehsana district. Three deaths out of 27 suspected cases reads, at first glance, like a small monsoon-season cluster the state has firmly in hand.
It is worth slowing down on that reading. The 27 is not the outbreak, it is only the patients whose samples had been fully processed by that evening, and even that group still had eight results outstanding. The number that carries the real story is not three deaths. It is seven: of 27 samples tested, only seven, just over a quarter, actually came back confirmed positive for Chandipura virus.
Confirmation is the bottleneck, and it is not new. In the 245-case, 82-death outbreak concentrated in Gujarat between June and mid-August 2024, the largest such outbreak in the past 20 years according to the World Health Organisation's Disease Outbreak News, India's national referral laboratory for the virus, NIV Pune, received 70 encephalitis samples and confirmed only 14 of them as Chandipura positive, 11 by PCR and three by antibody test, a confirmation rate of exactly one in five. Gujarat's 2026 count, seven confirmed of 27 tested, works out to about one in four. Two outbreaks, two years apart, and the lab system is catching roughly the same narrow slice of suspected cases each time.
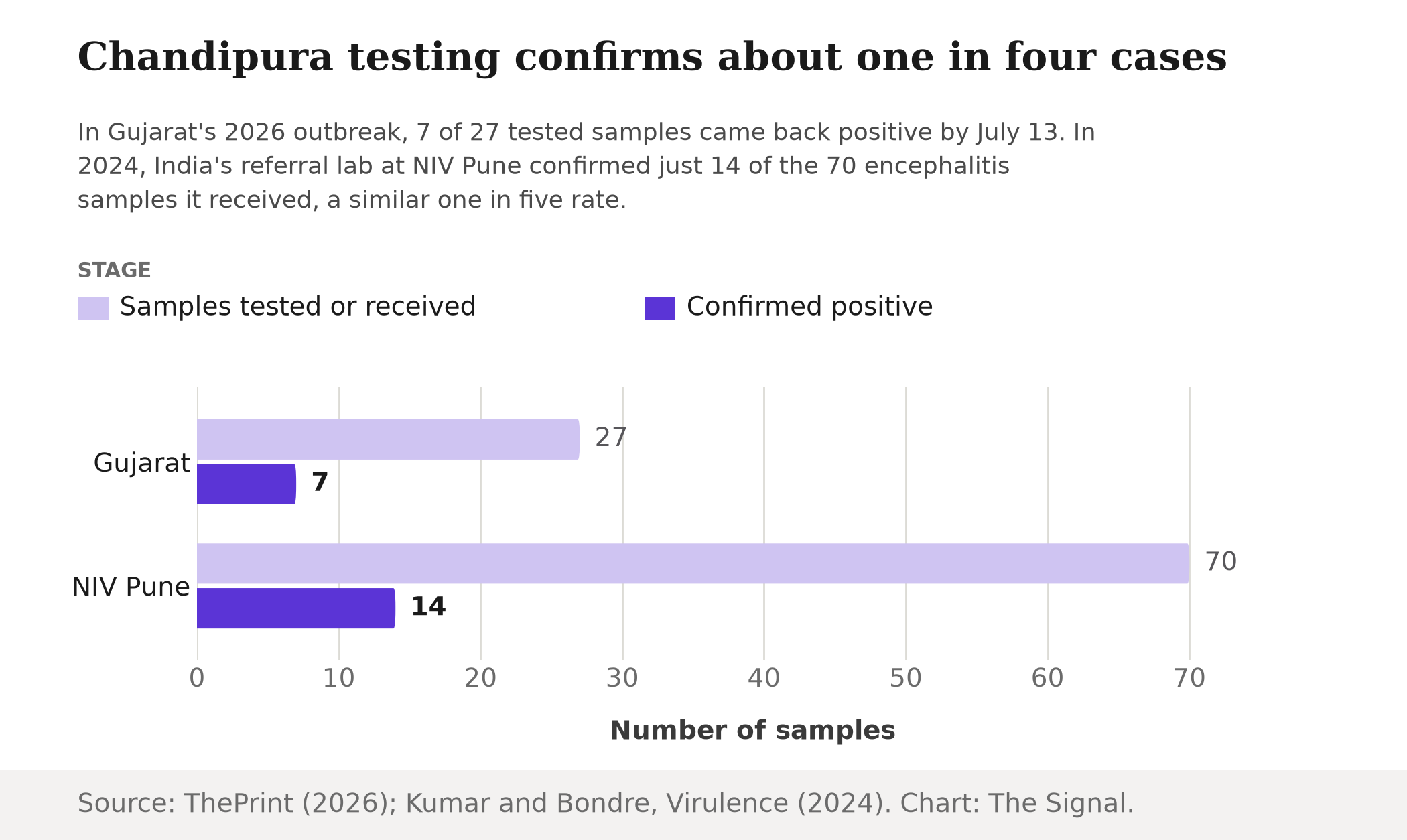
Source: ThePrint, July 13, 2026; Kumar and Bondre, Virulence, 2024. Chart: The Signal.
Why so few samples confirm
No licensed vaccine or antiviral treatment for Chandipura virus exists anywhere, and candidate drugs such as favipiravir remain in early, preclinical stages of development, with no completed human trials. That absence puts nearly the entire weight of the response on diagnosis and vector control, clearing sandfly breeding sites and spraying insecticide, rather than on treating patients once they are confirmed. Gujarat's health department says that approach has worked before: preventive spraying and awareness drives were completed at all 61 locations that reported Chandipura cases in 2024, and not a single new case has recurred at any of those 61 locations since. Fogging and sandfly-control spraying have already been launched in the areas newly affected in 2026. But diagnosis itself lags. A positive PCR or antibody result from NIV Pune, the country's central referral point for the virus, takes days to return, and children with acute encephalitis symptoms do not have days to spare. A 2024 systematic review of documented Chandipura outbreaks found case fatality rates ranging from 28.6% to 78.3% within the first 48 hours of symptom onset alone. A child can die before a pending result ever comes back.
Three outbreaks, one pattern
Seven Chandipura outbreaks have struck India since 2003, all clustering with the monsoon season, with case fatality rates recorded between 28% and 79% across them. The three largest, spread across more than two decades, still show the same signature: brutal fatality among the cases labs manage to confirm, and comparatively few confirmations relative to how many children fall ill.
Case fatality has stayed severe across three Chandipura outbreaks, over two decades apart.
| Outbreak | Cases | Deaths | Case fatality rate |
|---|---|---|---|
| 2003, Andhra Pradesh | 329 | 183 | 55.6% |
| 2024, Gujarat centred | 245 | 82 | 33% |
| 2026, Gujarat (confirmed so far) | 7 | 3 | 42.9% (our calculation) |
Source: Rao et al., The Lancet, 2004; WHO Disease Outbreak News, 2024; ThePrint, citing Gujarat's health department, July 13, 2026.
The 2003 outbreak in Andhra Pradesh, the one that first established Chandipura as a major pediatric killer, recorded 329 encephalitis cases and 183 deaths in children aged nine months to 14 years. Gujarat's 2026 figure of 42.9% sits between that 2003 peak and 2024's 33%, but it rests on just seven confirmed cases so far, a small enough base that a single additional death or recovery among the eight pending results would move it sharply in either direction.
Where the count stands now
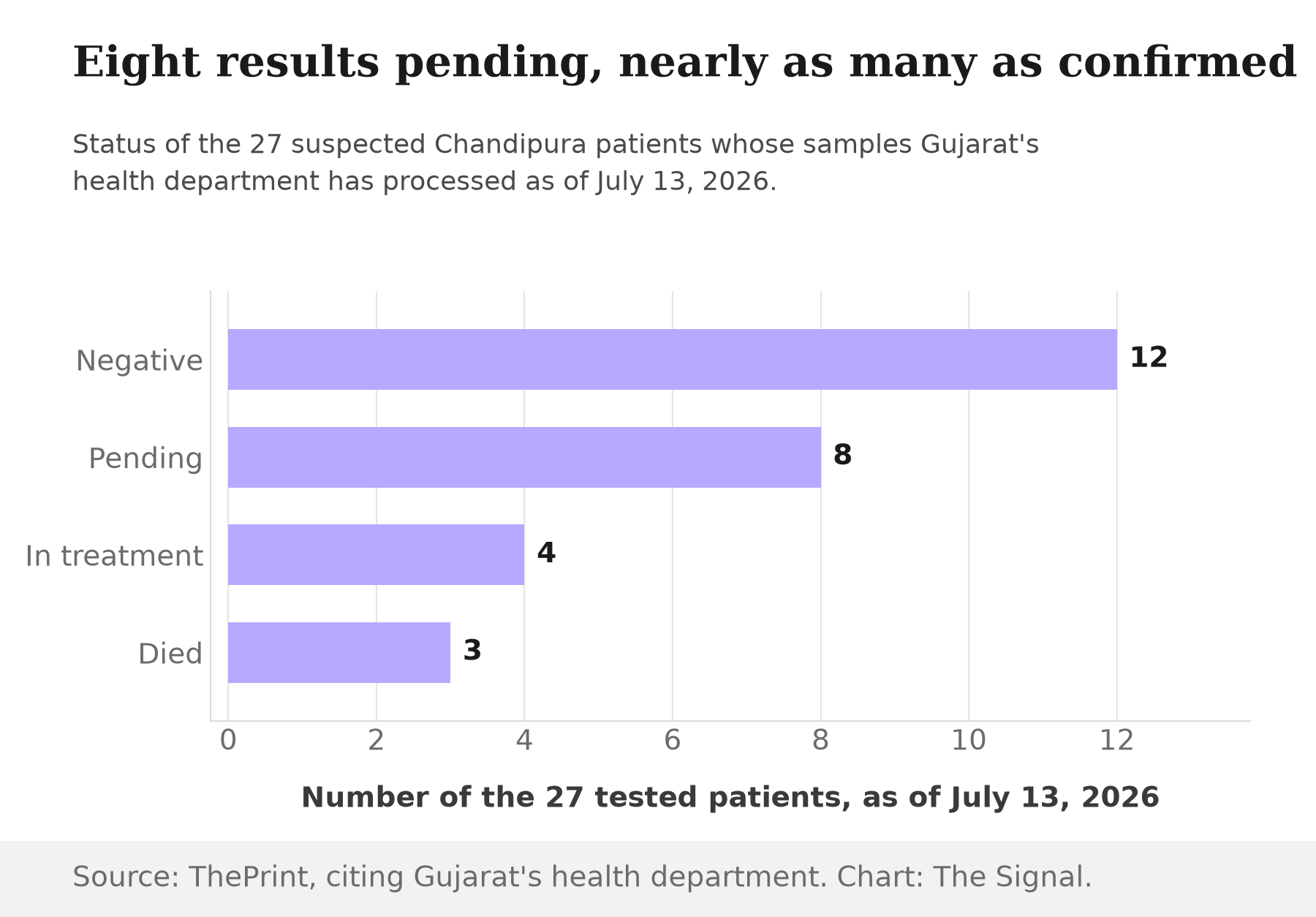
Source: ThePrint, July 13, 2026. Chart: The Signal.
Eight pending results is not a rounding error. It outnumbers the seven already confirmed positive, and the confirmed cases so far are concentrated in Gandhinagar and Vadnagar, Mehsana district. If those eight follow the same roughly one-in-four confirmation pattern the 2026 and 2024 outbreaks have both shown, two or three more could turn out positive. Given how front-loaded Chandipura fatality is within the first two days of symptoms, whether any of those additional confirmations arrive in time to matter is a separate question from whether they arrive at all.
The honest objection
The strongest case against reading too much into the confirmation gap is that three deaths in 2026 is a fraction of 2024's 82 or 2003's 183. Gujarat's health department is already reviewing the outbreak at ministerial level with 27 samples processed within weeks of the first cases, and most seasonal Chandipura scares in India do not become record-setting events. On that view, the low absolute numbers simply mean this outbreak is smaller, not that the state's diagnostic system is falling behind.
That case is real on scale, but it does not touch the actual finding here. The confirmation rate itself has held close to one in four in Gujarat's 2026 outbreak and one in five in NIV Pune's 2024 count, across two outbreaks two years apart and of very different size. That consistency is what makes it look structural rather than a one-off strain on lab capacity during an unusually large year. Whether this outbreak ends up small or turns into something closer to 2024's scale, a similar share of suspected cases is likely to go unconfirmed, and a similar share of deaths may occur before confirmation ever arrives.
The Signal
The number worth watching this week is not three deaths. It is whether the eight pending results move the confirmed count and the death toll, and whether that keeps happening at close to the same one-in-four, one-in-five rate the next time Chandipura returns with the monsoon. Without a vaccine or an approved antiviral, speed of diagnosis is nearly the only lever India has, and the lab system has not obviously gotten faster since 2024. A pending result is not a mild case. It is an unanswered question, and Chandipura does not wait long for answers.
Reporting basis: the 2026 Gujarat case, death and testing counts are as reported by ThePrint, citing the state health department's review chaired by health minister Praful Pansheriya. The 2024 outbreak's case and death toll is per the World Health Organisation's Disease Outbreak News, relaying figures from India's Ministry of Health and Family Welfare. NIV Pune's 2024 sample and confirmation counts are from a Virulence study by ICMR-National Institute of Virology scientists Kumar and Bondre. The 28.6 to 78.3 percent early case-fatality range is from a systematic review published in Cureus. The vaccine and antiviral development status is from a 2025 review in Global Health, Epidemiology and Genomics. The 2003 Andhra Pradesh outbreak figures are from Rao and colleagues' original Lancet report, and the count of seven outbreaks since 2003 is from a December 2024 review in Pathogens. The 2024 and 2026 vector-control figures are from Medical Dialogues, citing Gujarat health minister Praful Pansheriya's review meeting. Gujarat's 2026 case fatality rate and the one-in-four and one-in-five confirmation-rate comparisons are The Signal's calculations from those figures.


