
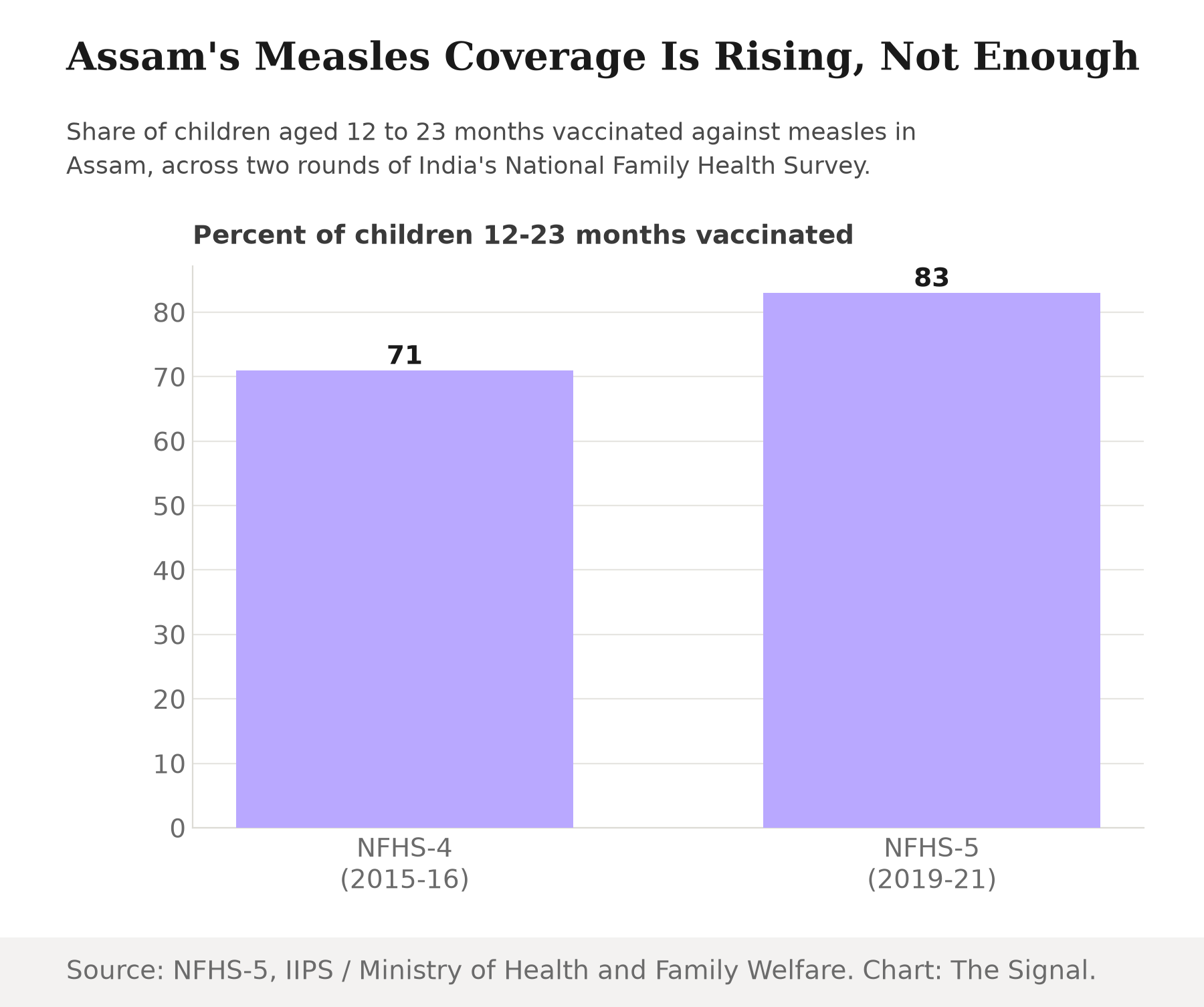
Assam's health department has a genuine improvement to point to. In the fifth round of India's National Family Health Survey, fielded across 2019 and 2021, NFHS-5 survey data show that 83 percent of the state's children aged 12 to 23 months had been vaccinated against measles, up from 71 percent in the prior NFHS-4 round, fielded in 2015-16. Twelve percentage points in five years is a real gain, and on a chart of the state's own history it reads as a program that is working.
It is worth slowing down on that framing. A coverage number only means something against a target, and measles does not grade on a curve. The World Health Organization's measles fact sheet states that one infected person can generate up to 18 secondary infections, among the highest transmissibility of any known human pathogen. Run that number through the standard epidemiological formula for herd immunity and the share of a population that needs immunity to break a chain of transmission comes out to roughly 94 percent, our calculation from the WHO's contagion figure. Assam's 83 percent sits about eleven points under that line. The state has not failed to improve. It has improved to a level that still leaves room for the virus to move.
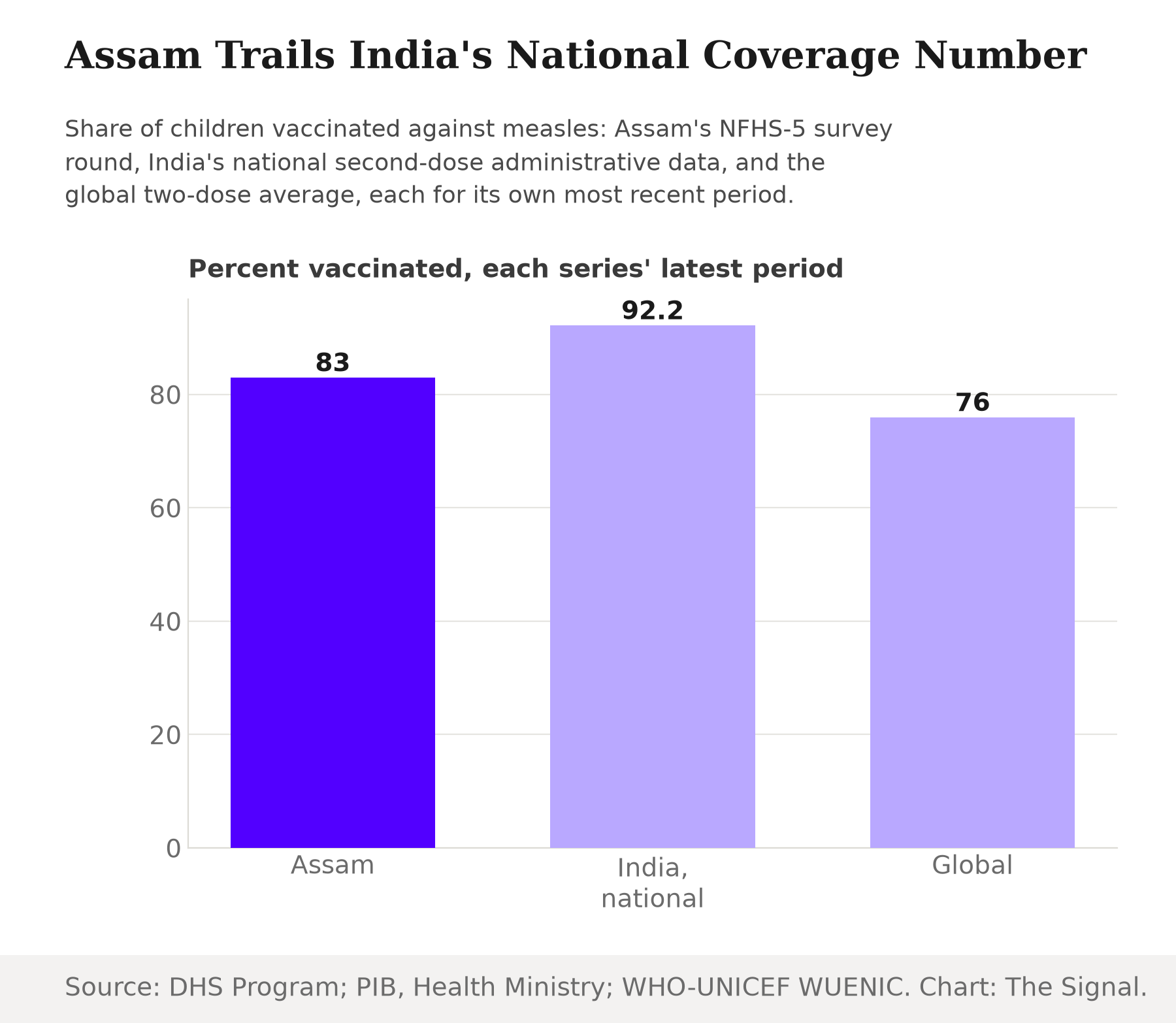
Assam trails India's own number, and the definitions do not match cleanly
Assam's shortfall looks smaller next to the rest of the world and larger next to the rest of India, and both comparisons need their fine print attached. The Press Information Bureau reports that India's measles-rubella vaccination coverage stood at 93.7 percent for the first dose and 92.2 percent for the second, per 2024-25 HMIS data from the Ministry of Health and Family Welfare. That is nine points above Assam's own survey figure, though the two are not measuring identically: Assam's 83 percent comes from a household survey asking parents about a child's vaccination card, while India's 92.2 percent comes from routine administrative reporting through the health system's own records, a method that tends to run higher than survey-based estimates.
Globally, the picture depends on which count is used. The World Health Organization reports that 76 percent of children received both recommended doses of measles vaccine by the end of 2024, which would put Assam ahead of the world average. But a 2025 study in the journal Vaccines put the global mean two-dose coverage at just 65.3 percent for 2023, a full ten points short of where WHO's own estimate landed a year later. The gap between those two numbers is a reminder that even a well-sourced global average moves with the survey wave and the counting method behind it, not only with what happened on the ground.
Bangladesh is the live test
None of this is theoretical two borders away. Bangladesh's outbreak has killed hundreds of children and adults, and its hospitals ran short of the beds to save them.
| Measure | Figure | As of |
|---|---|---|
| Suspected measles cases | 19,161 | 15 Mar-14 Apr 2026 |
| Laboratory-confirmed cases | 2,897 | 15 Mar-14 Apr 2026 |
| Deaths | 528 | 24 May 2026 |
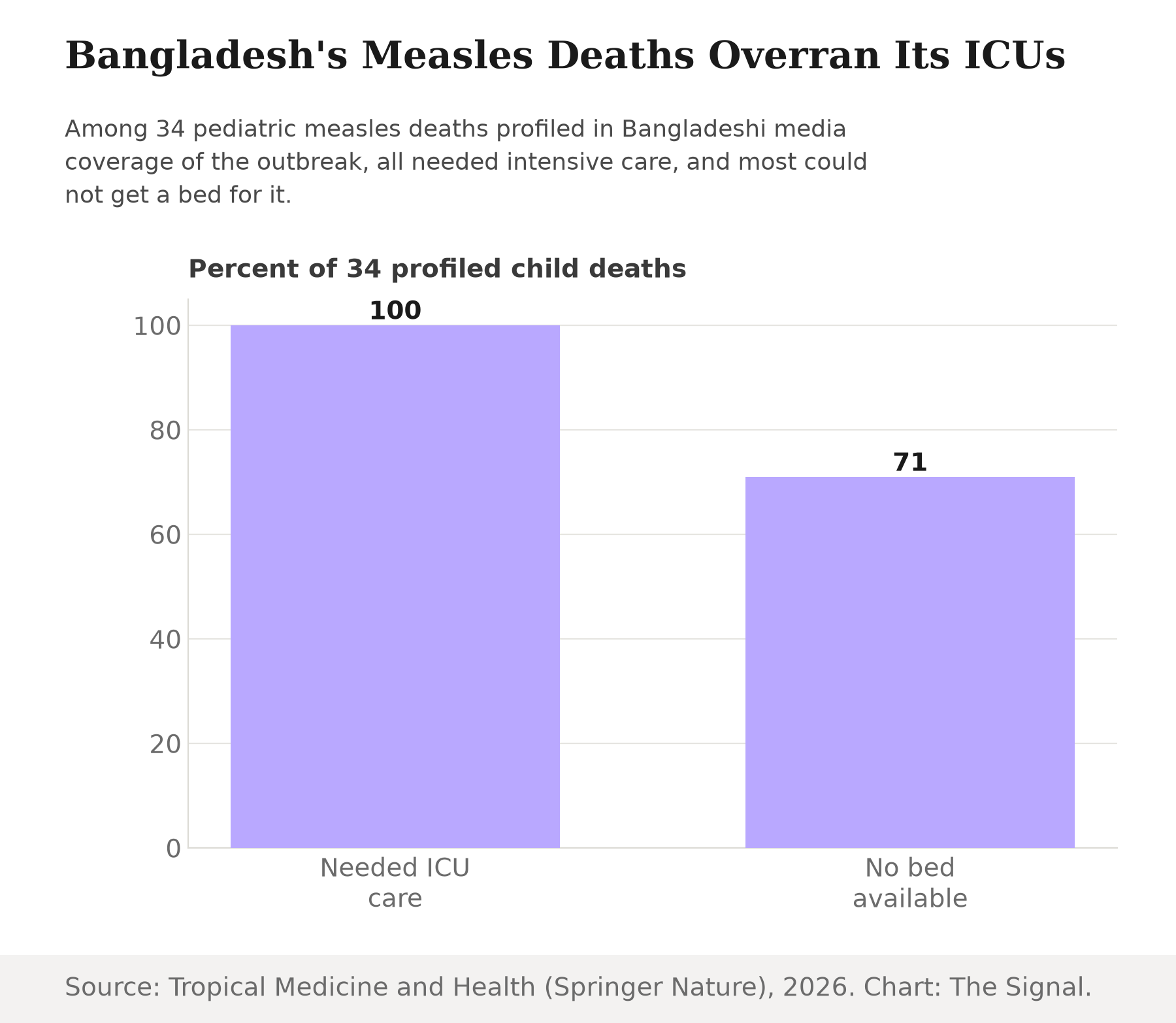
| Profiled child deaths that needed ICU or PICU care | 34 of 34 | 2026 |
| Those profiled deaths facing unavailable or full PICU beds | 71 percent | 2026 |
Source: World Health Organization, Disease Outbreak News; NPR; Tropical Medicine and Health. The Signal's compilation of the three reports.
The World Health Organization's Disease Outbreak News reports 19,161 suspected and 2,897 laboratory-confirmed measles cases in Bangladesh in the four weeks between 15 March and 14 April 2026 alone. NPR reported that the death toll had reached 528 as of 24 May 2026, already the largest measles outbreak in the country in decades. IANS reported that Bangladesh's Directorate General of Health Services put the combined confirmed-and-suspected toll at 758 as of 12 July 2026, a rise of 230 deaths in seven weeks and a toll still climbing as this piece goes to press. What the case count does not capture on its own is what happened once children got sick. A peer-reviewed analysis in Tropical Medicine and Health found that all 34 pediatric deaths profiled in Bangladeshi media coverage of the outbreak required ICU or PICU support, and 71 percent of them faced unavailable or fully occupied beds. Coverage below the threshold does not just raise the odds of an outbreak starting. It raises the odds that a hospital system built for a smaller caseload cannot save the children who get it.
The resurgence has not stayed on Bangladesh's side of the border, either. A World Health Organization India feature story describes a large, ongoing measles outbreak in Unakoti district, Tripura, active by late March 2026, a state that borders both Assam and Bangladesh. Assam itself has not reported an outbreak of that scale. But the virus this piece is tracking has already crossed into Indian territory next door, which is a different claim than a hypothetical risk two borders away.
The honest objection
The strongest case against reading Bangladesh as a preview of Assam's risk is that the two are not the same kind of event. Assam is not experiencing an active measles crisis right now, its national coverage figure is genuinely higher than Bangladesh's reported numbers, and the state's own trend line is improving, not stalling. It is also true that the global coverage figures above disagree by a wide margin depending on the source, which counsels some humility about precision at the decimal point. And a shortage of ICU beds is partly a hospital-capacity story, not only a vaccination story: even a country with strong coverage can be strained if an unrelated wave of respiratory illness lands in the same season.
That case is real, but it does not change the arithmetic that opened this piece. Herd immunity is not a spectrum where more coverage is proportionally better protection right up until an outbreak arrives to test it. Below the threshold, chains of transmission can still take hold and grow; above it, they cannot sustain themselves. Assam's 83 percent is short of that line, not by a rounding error, and Bangladesh's outbreak shows concretely what a population below the line looks like once the virus arrives: a caseload that outruns laboratory capacity and, in the most severe cases, an intensive care system with no beds left.
The Signal
Assam's health department can keep publishing a rising line, and it will not be wrong to do so. The number really did climb from 71 to 83 in five years. But a rising line and a sufficient line are different claims, and the gap between them is not academic once a virus this contagious is circulating in the region. The 94 percent threshold is not a target Assam missed by a little; it is the point past which the virus runs out of new children to infect, and 83 percent is not that point. Bangladesh's hospitals are the preview of what happens in the space between those two numbers. The question for Assam is not whether its coverage is rising. It is whether it clears 94 before the next outbreak asks the same question Bangladesh just answered.
Reporting basis: Assam's NFHS-4 and NFHS-5 measles coverage figures are from the National Family Health Survey's Assam state report, published by the International Institute for Population Sciences and the Ministry of Health and Family Welfare via The DHS Program. India's national measles-rubella coverage is 2024-25 HMIS data from the Ministry of Health and Family Welfare, via a Press Information Bureau release. The global two-dose estimates come from two distinct origins that disagree, WHO/UNICEF's WUENIC estimates and a 2025 Vaccines journal study, and are presented separately rather than pooled. Bangladesh's case and confirmed-case counts are from the World Health Organization's Disease Outbreak News; the death toll is as reported by NPR as of 24 May 2026 and updated using IANS's reporting of Bangladesh Directorate General of Health Services data as of 12 July 2026; the ICU and PICU bed findings are from a peer-reviewed analysis in Tropical Medicine and Health. The Unakoti, Tripura outbreak is from a World Health Organization India feature story. The measles reproduction-number figure is from the WHO's measles fact sheet. The herd-immunity threshold and the point-gap between Assam's coverage and that threshold are The Signal's calculations from those figures.


