
Zydus and Apollo are bringing Guardant Health's Shield blood test to Indian patients, pitching a simple blood draw as an easier alternative to a colonoscopy for catching colorectal cancer early. The pitch rests on a real number: Shield's pivotal ECLIPSE trial found the test correctly identified colorectal cancer 83.1% of the time, a result strong enough that the FDA cleared it in July 2024 as a primary screening option for average-risk adults. Read only that figure and a blood test that catches roughly 4 in 5 colorectal cancers looks like an obvious upgrade over asking healthy adults to book a colonoscopy.
It is worth slowing down on that number. Sensitivity, the 83.1% figure, only answers one question: if someone already has colorectal cancer, how often does the test catch it. It says nothing about what happens to everyone else, the overwhelming majority of any screening population, who do not have the disease. That second number is specificity, and it is the one that decides how a positive result actually behaves once the test leaves the trial and meets a real population.
For every 500,000 average-risk Indian adults screened, using Shield's published sensitivity and specificity against India's own colorectal cancer rate, about 22 real colorectal cancers get caught, and roughly 52,000 people test positive without having it.
Run Shield's own published numbers against India's own registry data, and a positive result is far more likely to be a false alarm than a real cancer.
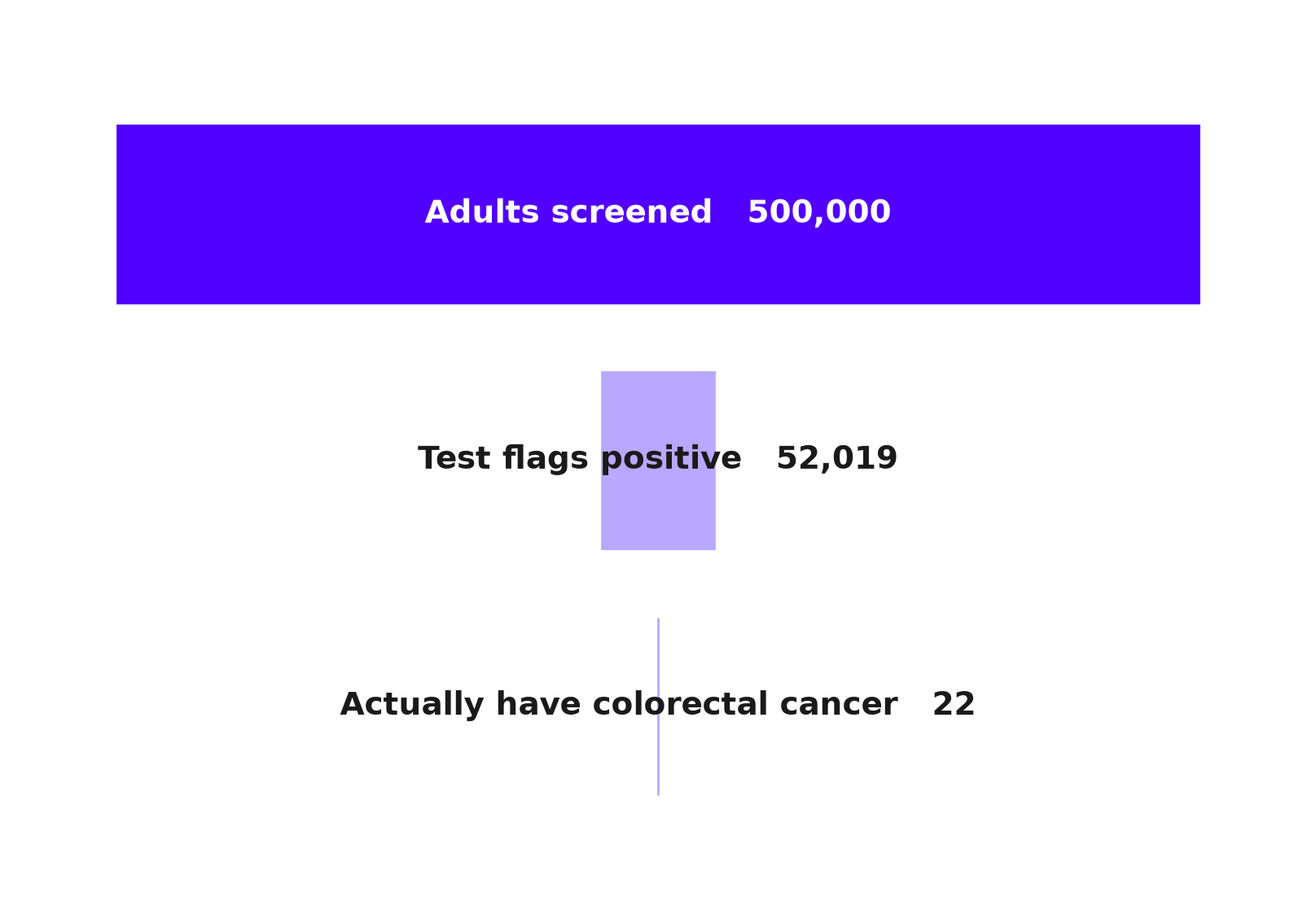
Source: ECLIPSE trial data, ECLIPSE specificity analysis, National Cancer Registry Programme, 2022. Chart: The Signal.
The number the trial result leaves out
A peer-reviewed analysis of the same ECLIPSE data reports Shield's specificity for advanced colorectal neoplasia at 89.6%, alongside the 83.1% sensitivity figure. Specificity is the mirror of sensitivity: it measures how often the test correctly comes back negative in people who do not have advanced neoplasia, a category that covers both cancer and advanced precancerous lesions. An 89.6% specificity means roughly 10.4% of people who do not have advanced neoplasia will still test positive.
That 10.4% sounds small next to 83.1%. It is not small once it is applied to a population where the disease is rare, which describes any general screening rollout. India's National Cancer Registry Programme estimates 38,107 new colon cancer cases and 38,752 new rectal cancer cases in 2022, a combined crude rate of 5.3 per 100,000 people (our calculation, summing the two site-specific rates the registry reports separately). Out of every 500,000 average-risk adults, only about 27 actually have colorectal cancer. Everyone else, all 499,973 of them, is exactly the group the 10.4% false-positive rate applies to.
Running the arithmetic
The math is basic Bayes, but it is exactly the calculation a screening rollout has to survive. Sensitivity tells you how many of the roughly 27 true cases the test catches: 27 times the trial's 83.1% sensitivity is about 22 correctly flagged, with about 5 missed. Specificity tells you how many of the 499,973 disease-free people still test positive. The trial's 89.6% specificity means a 10.4% false-positive rate, and 499,973 times that rate is about 51,997 false alarms (our calculation, applying the trial's published rates to the registry's population figures). Add the true and false positives together and the test returns roughly 52,019 positive results from that population of 500,000, of which only 22 are real cancer.
That works out to about 1 real cancer for every 2,362 positive results, using the same sensitivity and specificity figures applied above, or put the other way, roughly 2,361 false alarms for every cancer the test actually finds. Each of those 52,000 people would need a follow-up colonoscopy, the very procedure Shield is being marketed as sparing patients from, to find out they do not have cancer.
What the test misses even when the arithmetic works
The false-alarm math is not the only place Shield's accuracy is uneven. The same ECLIPSE data show sensitivity for advanced precancerous polyps at just 13.2%, against 83.1% for cancer itself.
The test is more than six times better at spotting cancer than at spotting the polyps that would let a doctor stop it before it becomes cancer.
Colonoscopy's real preventive value is catching and removing precancerous polyps years before they turn malignant. A blood test that identifies cancer well but the earlier warning signs poorly is answering a different, later question.
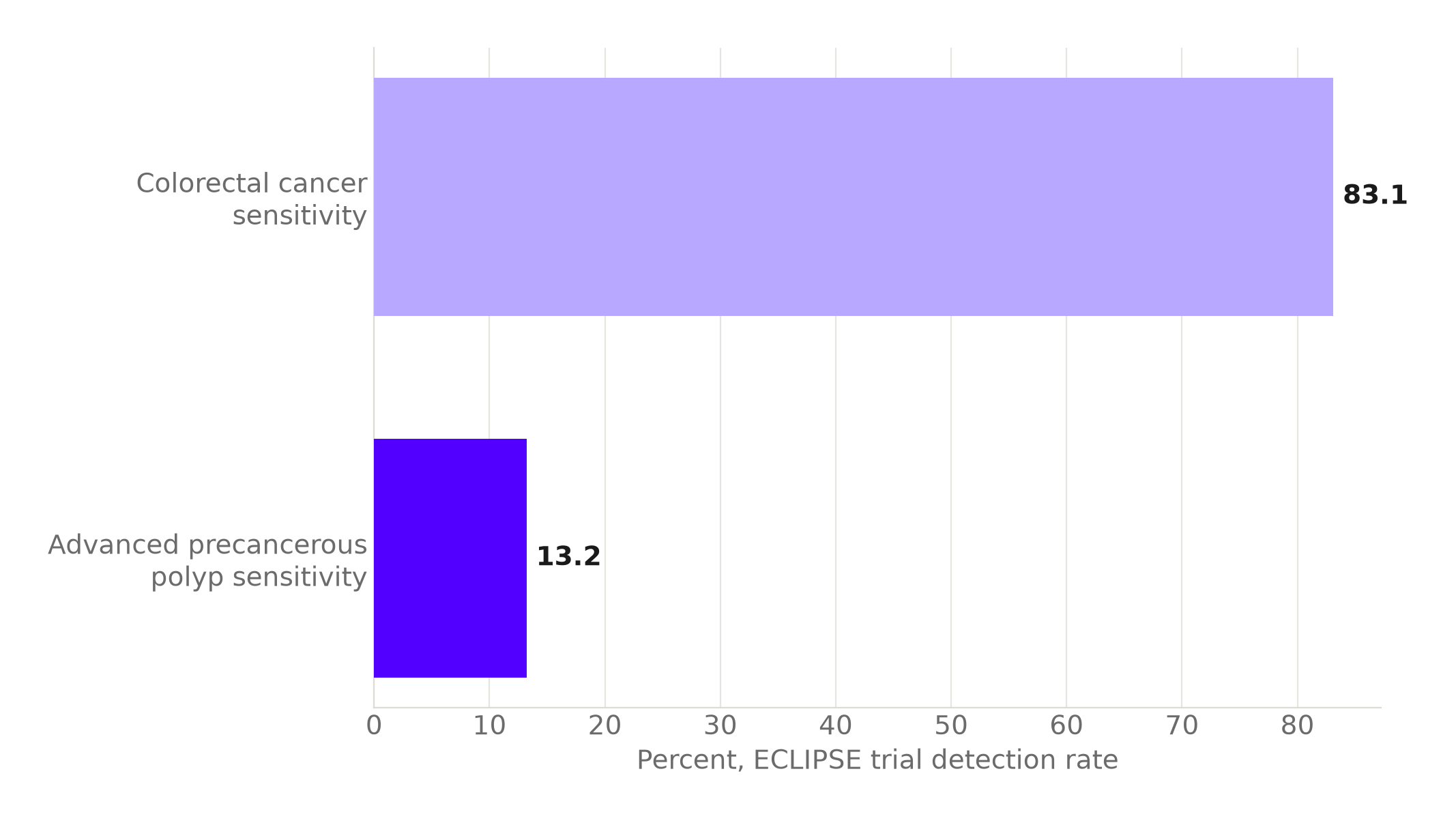
Source: Peer-reviewed ECLIPSE trial analysis. Chart: The Signal.
The test is also weakest exactly where early detection matters most. Memorial Sloan Kettering Cancer Center reports that Shield detected only 65% of Stage I colorectal cancers, the earliest and most curable stage screening exists to catch, missing 35% of them in the ECLIPSE trial.
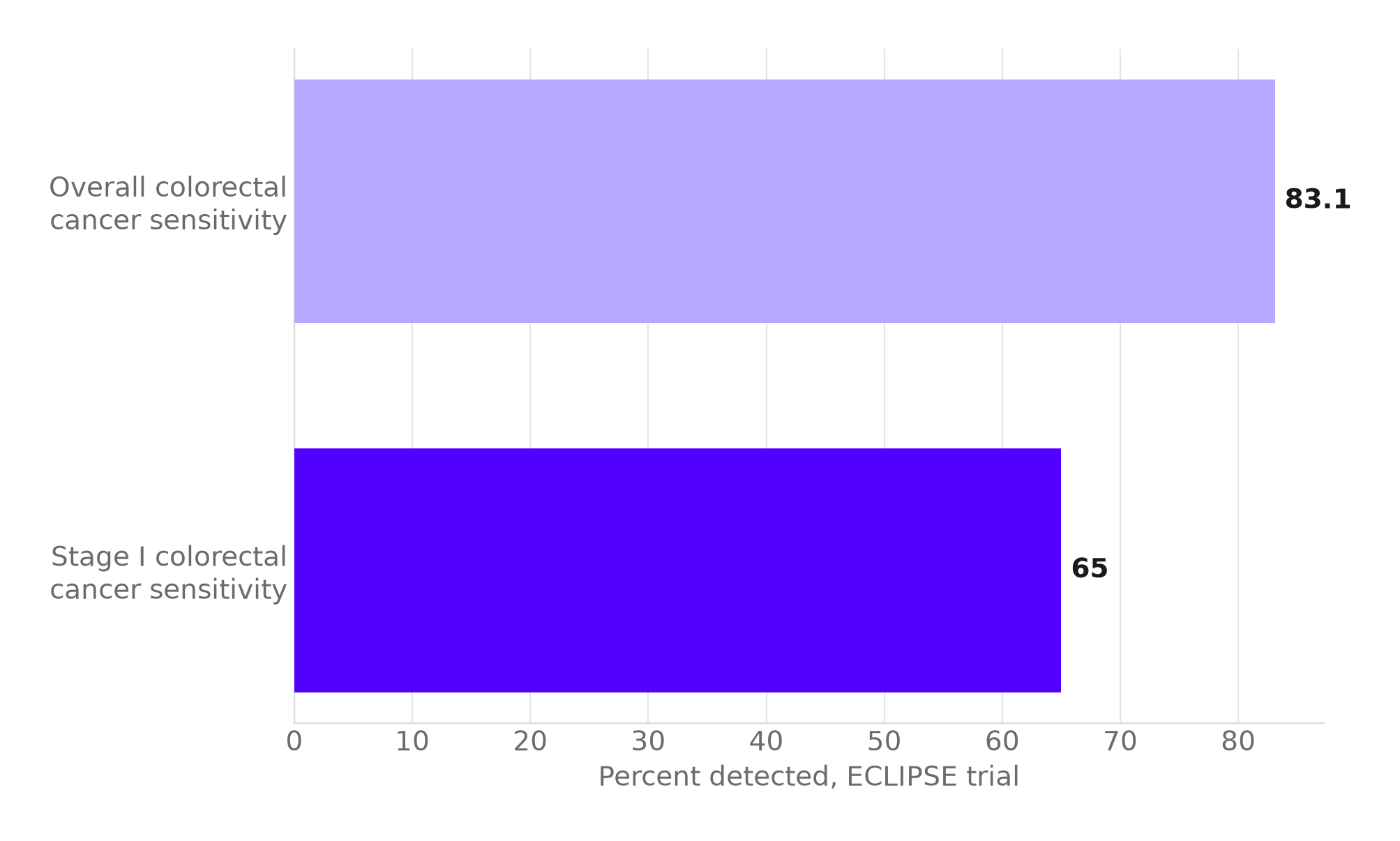
Source: Memorial Sloan Kettering Cancer Center, citing the ECLIPSE trial. Chart: The Signal.
The honest objection
The strongest case for Shield is that a blood draw beats no screening at all, and colonoscopy compliance in a general population is poor: many people who would never book an invasive procedure will still agree to a blood test. On that view, catching 22 real cancers per 500,000 people who otherwise get no screening is a genuine gain, and a positive Shield result was never meant to be a diagnosis, only a trigger for the confirmatory colonoscopy that follows. The false positives are a cost of that trigger, not a failure of it.
That case holds up for the cases the test does catch. It does not change the scale of the false-alarm math itself: 52,000 unnecessary follow-up colonoscopies for every 22 real cancers found is a real burden on India's endoscopy capacity and on the anxiety of the people who wait for that follow-up, and it says nothing about the 35% of Stage I cancers and the 86.8% of advanced precancerous polyps, the complement of the trial's 13.2% precancerous-polyp sensitivity, the test misses entirely. A test can be worth deploying and still be far less accurate, in practice, than its headline sensitivity number suggests.
The Signal
Shield's 83.1% sensitivity is a real, peer-reviewed number. So is the arithmetic that turns it, once applied to a population where colorectal cancer runs at 5.3 per 100,000, into a positive result that is right about 1 time in 2,362. Neither number is wrong; they are answering different questions, and only one of them tells a patient what a positive result on their own report actually means. As Zydus and Apollo roll Shield out to Indian patients, the number worth watching is not the sensitivity on the label. It is how many of the follow-up colonoscopies it triggers turn out to be for nothing.
Reporting basis: Shield's FDA clearance and its headline sensitivity for colorectal cancer and precancerous polyps are per the National Cancer Institute, restating the FDA-reviewed trial data. The precise sensitivity, specificity and precancerous-polyp detection figures from the ECLIPSE trial are from a peer-reviewed report of that trial and a separate peer-reviewed analysis of the same trial data. The Stage I detection figure is per Memorial Sloan Kettering Cancer Center's reporting of the ECLIPSE results, a single secondary source for that specific figure. India's colorectal cancer incidence and crude rate are from the National Cancer Registry Programme's official 2022 estimates, published in the Indian Journal of Medical Research. The combined colon-and-rectum crude rate, the per-500,000-population case counts, the true and false positive counts, and the resulting positive predictive value are The Signal's calculations from those figures.


