
India's sixth National Family Health Survey put the country's caesarean-section rate at 27.2 percent of institutional births in 2023-24, up from 21.5 percent in 2019-21, according to the Ministry of Health and Family Welfare's NFHS-6 fact sheet. The World Health Organization has held since 1985 that the ideal caesarean rate is 10 to 15 percent of births, the point past which more surgery buys no further improvement in maternal or infant survival. The obvious read is that India's rate has drifted roughly double the point doctors consider medically justified, and that the drift tracks a country where mothers are older, heavier and more likely to carry a pregnancy complication than a decade ago.
It is worth slowing down on that reading before accepting it. The national number hides a split that has nothing to do with any single mother's risk profile. In the same NFHS-6 data, 54.1 percent of births in private hospitals were delivered by caesarean section, against 16.9 percent in public hospitals, a gap of roughly 3.2 times. Private and public hospitals in India are not treating two different populations of women. A mother's odds of leaving with a surgical scar instead of a vaginal delivery depend enormously on which kind of building she walks into.
Private hospitals in India run caesareans at more than triple the rate of public ones.
This is a split by which kind of hospital delivered the baby, not by how sick the mother was.
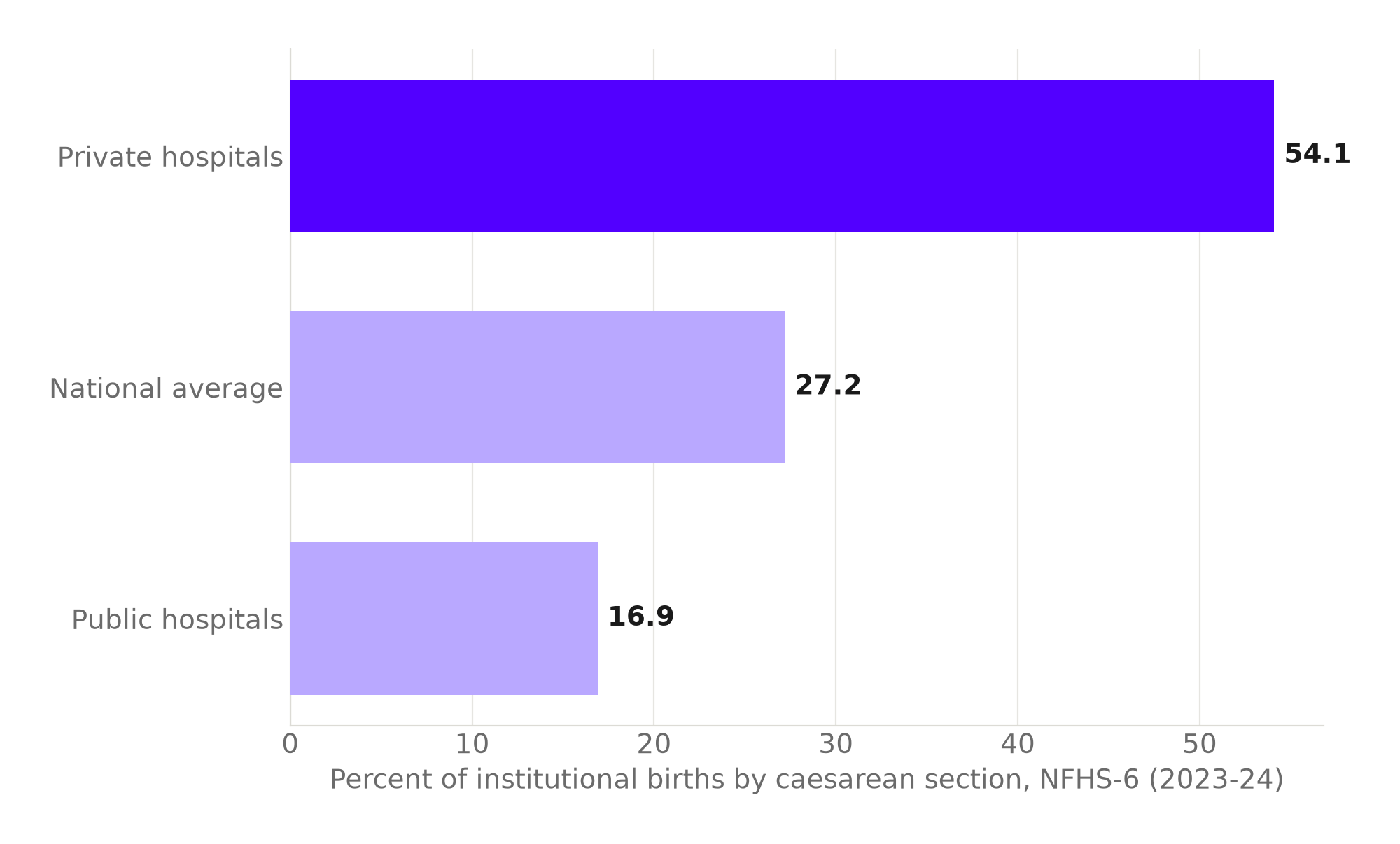
Source: The South First, citing NFHS-6 data. Chart: The Signal.
The figure that actually carries the story is smaller and sharper than either of the headline rates. A peer-reviewed analysis of NFHS-5 data found that mothers delivering at a private facility had 2.9 times the odds of a preventable caesarean section compared with mothers at public facilities. Not a caesarean section, full stop. A preventable one, by the study's own clinical criteria for when surgery wasn't medically indicated. That is not a description of sicker patients. It is a description of a system.
The natural experiment India already ran
The clean way to separate "sicker patients go private" from "private hospitals are paid to operate" is to change how a hospital gets paid and watch what happens to the same population. India ran that experiment, without realizing it, across two states in the same decade. Under Madhya Pradesh's Janani Sahayogi Yojana, which paid private obstetricians more for performing a caesarean section than for a vaginal delivery, the state's caesarean rate rose from 26.6 percent in 2007-08 to 40.7 percent by 2010-11. Over the same window, Gujarat ran a flat-fee scheme, the Chiranjeevi Yojana, that paid the same amount regardless of delivery method, and its caesarean rate fell to 4.3 percent by 2010-11, down from a background rate of 8.1 percent in 2004-06.
Two states, two fee schedules, opposite results within the same three years.
Paying more for surgery pushed the rate up. Paying the same regardless of method pushed it down. Nothing over that same window suggests Madhya Pradesh's mothers were suddenly sicker relative to Gujarat's; the incentive attached to the procedure changed instead.
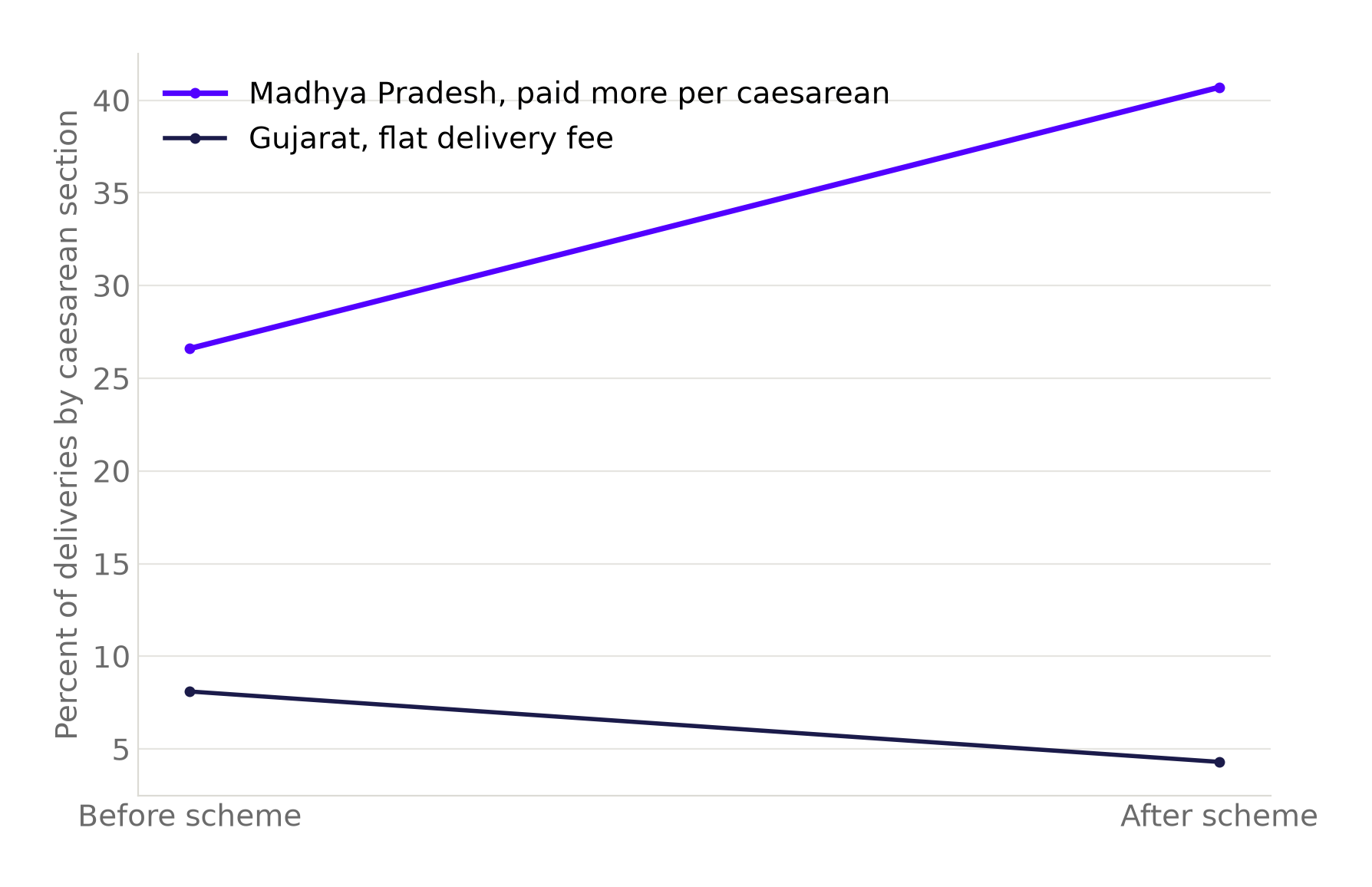
Source: Peer-reviewed study, Maternal and Child Health Journal. Chart: The Signal.
Insurance was supposed to fix this. It hasn't.
The standard policy answer to a cost-driven caesarean rate is to take cost out of the decision: give mothers cashless insurance so neither the hospital's bill nor the family's fear of it shapes the choice of delivery method. India has scaled exactly that answer through PMJAY, its flagship public health insurance scheme, and a wider set of publicly-funded health insurance programs. A peer-reviewed study using NFHS-5 data found that enrollment in PMJAY or other publicly-funded health insurance was not associated with any reduction in out-of-pocket spending on caesarean or non-caesarean institutional deliveries anywhere in India. The same study put caesarean deliveries at 49.5 percent of institutional births in private hospitals against 15.5 percent in public hospitals, nearly 3.2 times, confirming the NFHS-6 gap in an independent dataset one survey round earlier.
Cashless insurance was meant to neutralize the financial incentive at the point of care. It hasn't, because the incentive it was designed to remove sits with the hospital and the treating doctor, not with the paying family. A scheme that reimburses a facility more generously for a caesarean than a vaginal birth, or that simply pays out regardless of clinical necessity, leaves the underlying calculation exactly where it was.
How India's private rate compares abroad
None of this makes India unique in worrying about caesarean rates drifting from clinical need. The United States' own cesarean delivery rate rose to 32.3 percent of all births in 2023, its highest level in a decade, according to the CDC's final birth data, a system with its own long-running debate over fee-for-service obstetric incentives. But India's private-hospital rate of 54.1 percent runs well past even that American high-water mark. The country's public hospitals, at 16.9 percent, sit close to the WHO's ceiling; its private hospitals sit more than three and a half times above it.
| Population | Caesarean rate | Source, as of |
|---|---|---|
| WHO recommended ceiling | 10-15% | WHO, standing guidance since 1985 |
| India, public hospitals | 16.9% | NFHS-6, 2023-24 |
| India, national average | 27.2% | NFHS-6, 2023-24 |
| United States, all births | 32.3% | CDC, 2023 |
| India, private hospitals | 54.1% | NFHS-6, 2023-24 |
Source: WHO; NFHS-6 via The South First; CDC National Vital Statistics Reports. Table: The Signal.
The honest objection
The strongest case against reading this as pure incentive is that private hospitals may simply see a different, higher-risk population: older mothers, first-time mothers past a certain age, more pre-existing conditions like gestational diabetes or hypertension, concentrated in the urban centers where private maternity care clusters. On that view, the gap simply reflects which kind of patient walks through each door, not how that door gets paid.
That case weakens against a state that ran the opposite experiment inside its own public system. In Bihar, one of India's lowest-caesarean states, the caesarean rate at public facilities fell from 8.2 percent in 2015 to 2.1 percent in 2019, even as the state's overall caesarean rate rose from 6.2 percent to 9.7 percent over the same four years. If rising maternal risk were driving the state's climbing rate, it should show up inside public hospitals too, since they serve the same population getting older and sicker. Instead the public-sector rate moved the opposite direction, sharply, while the state total climbed on the strength of the private sector alone.
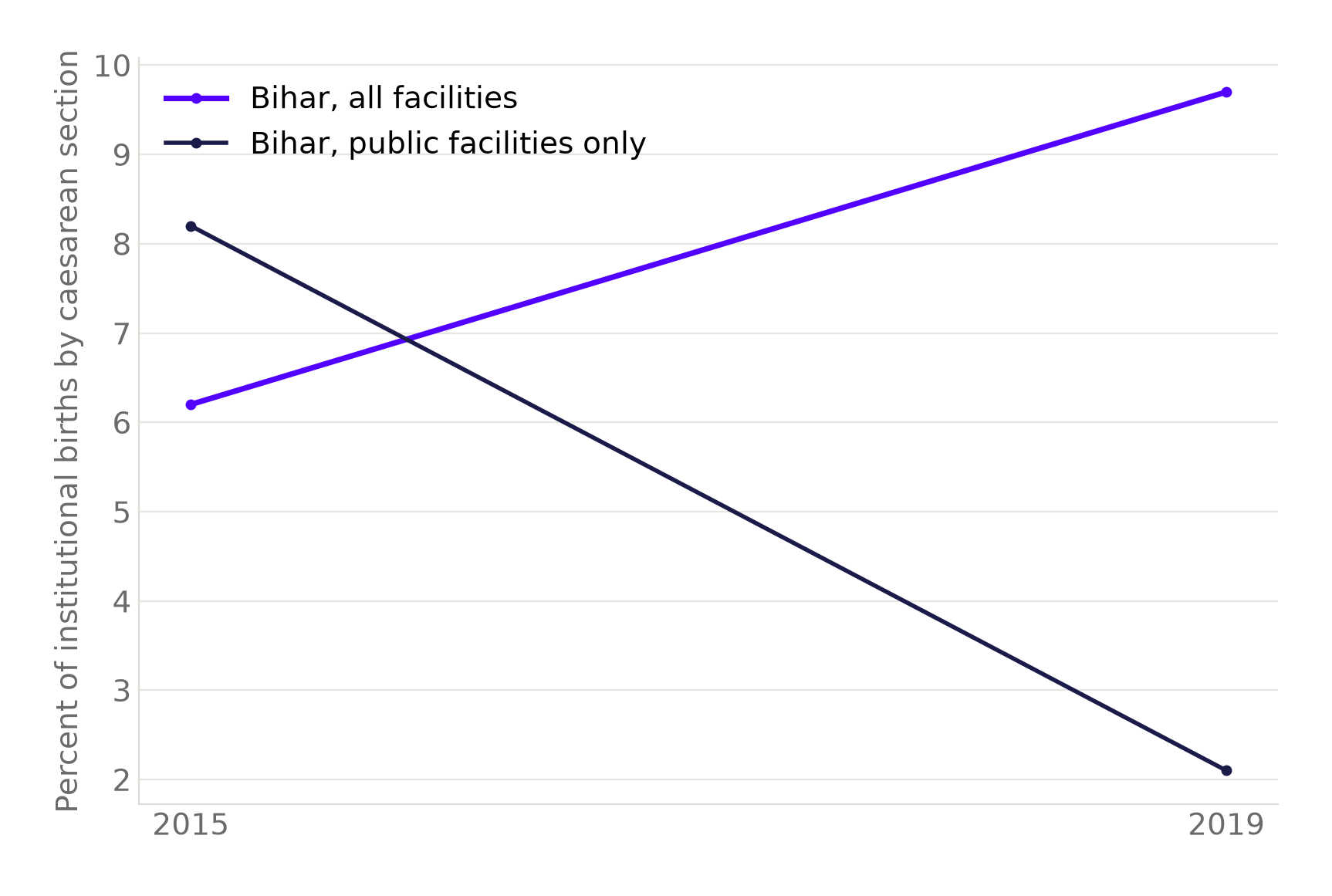
Source: Peer-reviewed secondary analysis of NFHS district data. Chart: The Signal.
The Signal
India's caesarean-rate debate is often framed as a medical question: are more mothers genuinely at risk. The strongest evidence against that framing is not medical at all, it is a payment schedule. Madhya Pradesh and Gujarat ran the same window with the same broad population and produced opposite trend lines because one state's fee schedule rewarded surgery and the other's didn't. Bihar's public hospitals sharply cut their own caesarean rate while the state total climbed, inside that same window, under the same disease burden. PMJAY shows that cashless insurance alone doesn't touch the underlying incentive, because the incentive was never the family's to remove. Watch what regulators do next, not what they say: a state or insurer that ties reimbursement to a documented clinical indication, rather than to the procedure performed, is the one policy lever this evidence says will actually move the needle. Everything else is a conversation focused on mothers, aimed at a problem that lives with the hospital.
Reporting basis: the national caesarean rate is from the Ministry of Health and Family Welfare's own NFHS-6 fact sheet; the private-versus-public split within that same round is per The South First's coverage. The preventable-caesarean odds ratio and the Bihar public-versus-overall divergence each come from a separate peer-reviewed analysis of that same underlying government dataset. The Madhya Pradesh and Gujarat payment-scheme comparison and the PMJAY out-of-pocket and facility-type findings each come from their own peer-reviewed journal article. The World Health Organization benchmark is the organization's own standing guidance, and the American figure is from the CDC's final 2023 birth-data release. The private-to-public multiples, and the comparison of the private-hospital rate against the international ceiling described above, are The Signal's own calculations from those underlying figures.


